Dong Liang, Lu Cao, Wensen Chen, Fuzhong Chen, Khalid Muhammad, Xiaoyu Dong, Guangjuan Li, Yanxia Qian, Yufeng Zhang, Xinjian Liu, Leilei Chen, Junhong Wang
Department of Cardiology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China.
Office of Infection Management, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China.
Front Cardiovasc Med. 2022 Jul 8;9:910805. doi: 10.3389/fcvm.2022.910805. eCollection 2022.
Recently, the Age-Bleeding-Organ Dysfunction (ABO) algorithm was recommended by the Asian Pacific Society of Cardiology Consensus as a binary approach to evaluate bleeding risk. This analysis made comparison of the predictive performances between the PRECISE-DAPT and ABO bleeding score in identifying the risk of 12-months major bleeding in Chinese elderly patients over 65 years old patients who underwent percutaneous coronary intervention (PCI) during dual-antiplatelet therapy period.
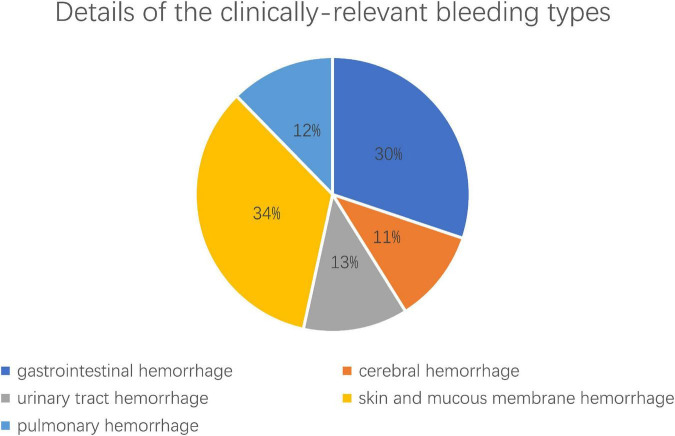
A total of 2,037 elderly coronary artery disease (CAD) patients (≥65 years) receiving dual antiplatelet therapy (DAPT) after PCI were enrolled in the study. The predictive accuracy of the two bleeding risk scores (PRECISE-DAPT and ABO) was compared for identifying the risk of bleeding during the dual-antiplatelet therapy in patients who underwent PCI. Major clinically relevant bleeding events were defined according to the Bleeding Academic Research Consortium (BARC) criteria.
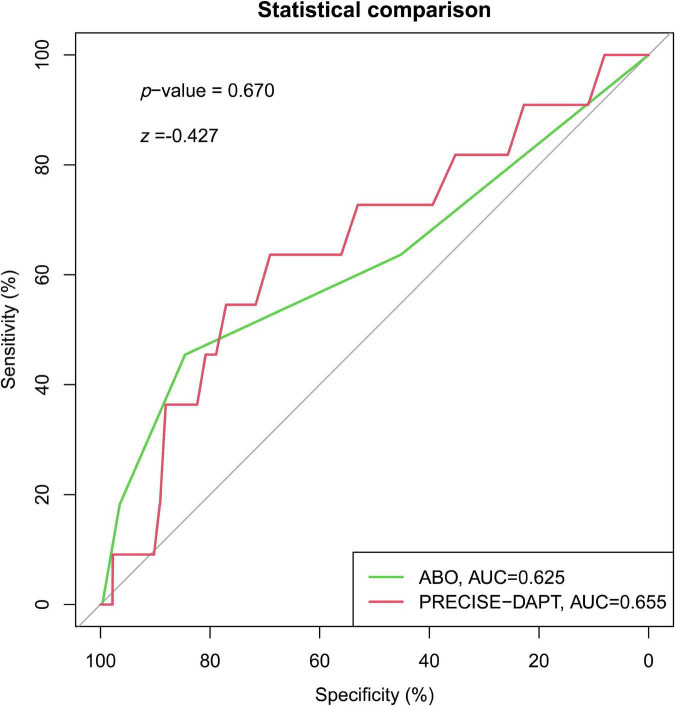
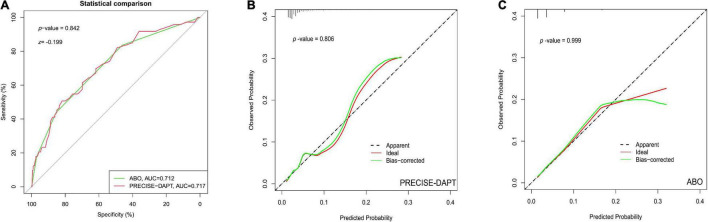
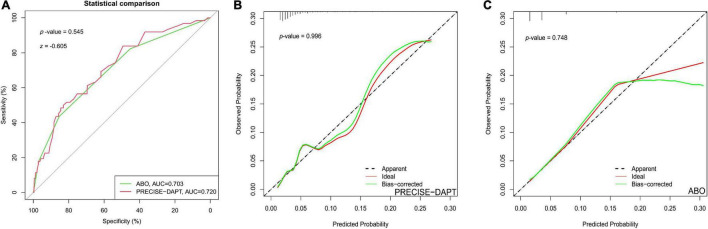
The PRECISE-DAPT score in the no bleeding, BARC = 1 bleeding, BARC ≥ 2 bleeding patients was 23.55 ± 10.46, 23.23 ± 10.03, and 33.54 ± 14.33 ( < 0.001), respectively. Meanwhile, the ABO score in the three groups was 0.72 ± 0.80, 0.69 ± 0.81, and 1.49 ± 0.99 ( < 0.001), respectively. The C-statistic of the PRECISE-DAPT model for prediction of BARC ≥ 2 bleeding in overall patients was 0.717 (95% CI, 0.656-0.777) and 0.720 (95% CI, 0.656-0.784) in acute coronary syndrome (ACS) patients. Similar discriminatory capacity was demonstrated in the ABO risk score [overall, patients, AUC: 0.712 (95% CI, 0.650-0.774); ACS patients, AUC: 0.703 (95% CI, 0.634-0.772)]. No differences were observed when the ABO model was in comparison with the PRECISE-DAPT model, regardless in overall patients ( = -0.199, = 0.842) or ACS patients ( = -0.605, = 0.545). The calibration for BARC ≥ 2 bleeding of the PRECISE-DAPT and ABO score were acceptable, regardless in overall patients [goodness-of-fit (GOF) Chi-square = 0.432 and 0.001, respectively; -value = 0.806 and 0.999, respectively] or ACS patients (GOF Chi-square = 0.008 and 0.580, respectively; -value = 0.996 and 0.748, respectively).
No matter of clinical presentation in Asian 65-years older patients with DAPT, the PRECISE-DAPT, and ABO scores had the similar discriminative ability for 12-months BARC ≥ 2 bleeding. Considering the simplicity and reliability, the PRECISE-DAPT score might be more clinically applicable in the overall population and ACS patients in bleeding prediction.
最近,亚太心脏病学会共识推荐采用年龄-出血-器官功能障碍(ABO)算法作为评估出血风险的二元方法。本分析比较了PRECISE-DAPT评分与ABO出血评分在识别65岁以上接受经皮冠状动脉介入治疗(PCI)的中国老年患者双联抗血小板治疗期间12个月大出血风险方面的预测性能。
本研究共纳入2037例PCI术后接受双联抗血小板治疗(DAPT)的老年冠状动脉疾病(CAD)患者(≥65岁)。比较了两种出血风险评分(PRECISE-DAPT和ABO)在识别PCI术后患者双联抗血小板治疗期间出血风险的预测准确性。主要临床相关出血事件根据出血学术研究联盟(BARC)标准定义。
无出血、BARC=1级出血、BARC≥2级出血患者的PRECISE-DAPT评分分别为23.55±10.46、23.23±10.03和33.54±14.33(<0.001)。同时,三组患者的ABO评分分别为0.72±0.80、0.69±0.81和1.49±0.99(<0.001)。PRECISE-DAPT模型预测总体患者BARC≥2级出血的C统计量为0.717(95%CI,0.656-0.777),急性冠状动脉综合征(ACS)患者为0.720(95%CI,0.656-0.784)。ABO风险评分显示出相似的鉴别能力[总体患者,AUC:0.712(95%CI,0.650-0.774);ACS患者,AUC:0.703(95%CI,0.634-0.772)]。与PRECISE-DAPT模型相比,ABO模型在总体患者(P=-0.199,P=0.842)或ACS患者(P=-0.605,P=0.545)中均未观察到差异。PRECISE-DAPT评分和ABO评分对BARC≥2级出血的校准是可接受的,无论是总体患者[拟合优度(GOF)卡方分别为0.432和0.001;P值分别为0.806和0.999]还是ACS患者(GOF卡方分别为0.008和0.580;P值分别为0.996和0.748)。
对于接受DAPT的亚洲65岁以上患者,无论临床表现如何,PRECISE-DAPT评分和ABO评分在预测12个月BARC≥2级出血方面具有相似的鉴别能力。考虑到简单性和可靠性,PRECISE-DAPT评分在总体人群和ACS患者的出血预测中可能更具临床适用性。