Department of Pancreatic Surgery, West China Hospital, Sichuan University, Chengdu, China.
The First Clinical College, Chongqing Medical University, Chongqing, China.
Front Endocrinol (Lausanne). 2022 Jul 6;13:907415. doi: 10.3389/fendo.2022.907415. eCollection 2022.
Small non-functional neuroendocrine tumors (NF-PNETs) are a heterogeneous subset of tumors with controversy regarding their optimal management. We aimed to analyze the prognostic factors of patients with small NF-PNETs and create a risk score for lymph node metastasis (LNM).
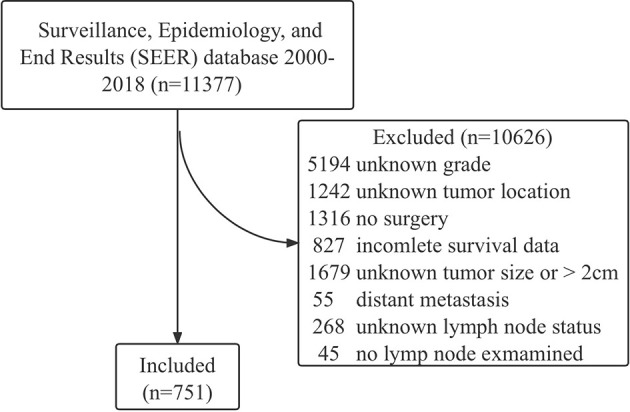
Data of 751 patients with NF-PNETs ≤ 2 cm were obtained from the Surveillance, Epidemiology, and End Results (SEER) database. Multivariate survival analysis was performed to analyze the prognostic factors. Logistic regression was used to identify risk factors for LNM.
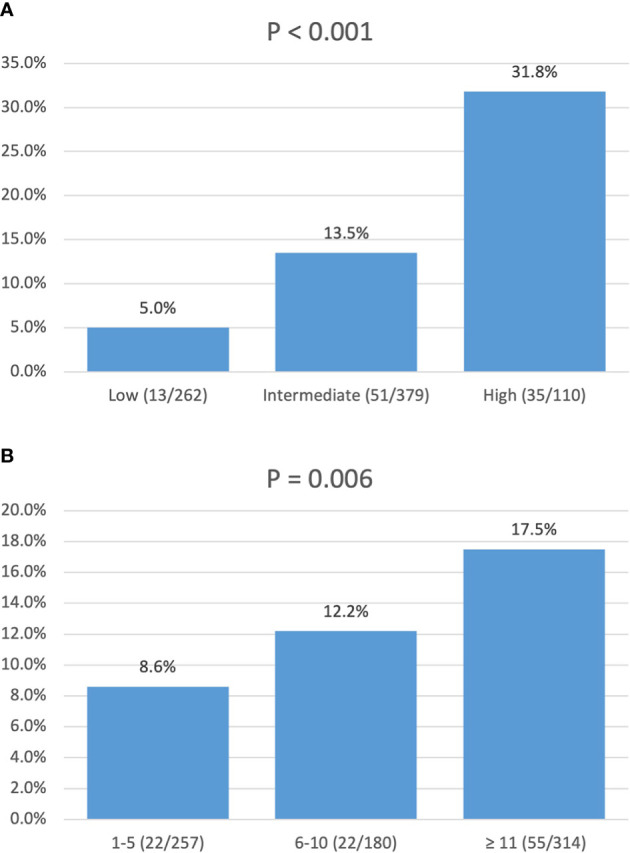
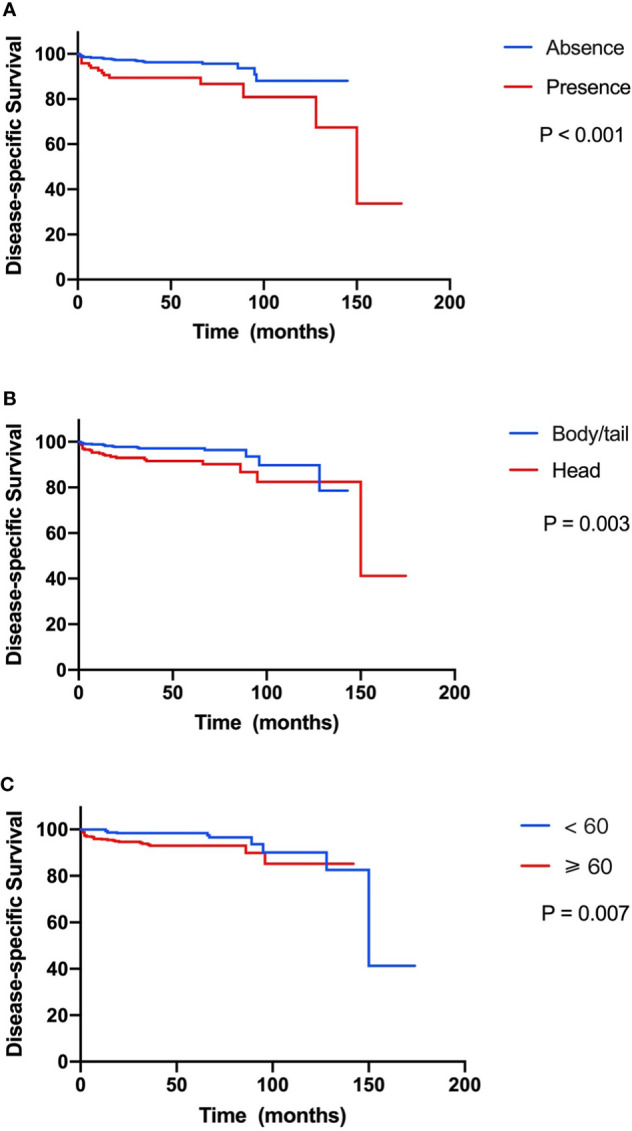
Of the 751 patients, 99 (13.2%) were confirmed to have LNM. In multivariate survival analysis, LNM (hazard ratio [HR], 2.12; 95% CI, 1.04-4.32, p = 0.040) was independently associated with disease-specific survival. Logistic regression identified that tumor location in the head of the pancreas (odds ratio [OR], 4.33; 95% CI, 2.75-6.81; p < 0.001), size ≥ 1.5-2 cm (OR, 1.84; 95% CI, 1.17-2.87; p = 0.009), and grade III-IV (OR, 7.90; 95% CI, 1.79-34.90; p = 0.006) were independent risk factors of LNM. According to the OR value, the risk of LNM was scored as follows: a score of 1 for tumors located in the body/tail of the pancreas and 4 for those located in the head; a score of 1 for tumors <1 cm and 2 for those ≥1.5-2 cm; and a score of 1 for tumors with grade I-II and 8 for those with grade III-IV. Finally, the median score for this cohort was 4, with an interquartile range of 3-6. Therefore, patients were classified as three groups based on the risk score system: a total score of 1-3 for low risk, 4-6 for intermediate risk (OR, 2.98; 95% CI, 1.59-5.60; p = 0.001), and 7-14 for high risk (OR, 8.94; 95% CI, 4.50-17.7; p < 0.001), with an incidence of LNM 5.0%, 13.5%, and 31.8%, respectively (p < 0.001).
Surgical resection with regional lymphadenectomy is recommended for small NF-PNETs with malignant potential of LNM. A risk score for LNM based on tumor grade, location, and size may preoperatively predict LNM of small NF-PNETs and guide clinical practice.
小的无功能性神经内分泌肿瘤(NF-PNETs)是肿瘤的一个异质亚组,其最佳治疗方法存在争议。我们旨在分析小 NF-PNET 患者的预后因素,并建立淋巴结转移(LNM)的风险评分。
从监测、流行病学和最终结果(SEER)数据库中获得了 751 例 NF-PNETs≤2cm 的患者数据。进行多变量生存分析以分析预后因素。使用 logistic 回归确定 LNM 的危险因素。
在 751 例患者中,99 例(13.2%)被证实有 LNM。多变量生存分析显示,LNM(风险比[HR],2.12;95%CI,1.04-4.32,p=0.040)与疾病特异性生存独立相关。logistic 回归确定肿瘤位于胰头(比值比[OR],4.33;95%CI,2.75-6.81;p<0.001)、大小≥1.5-2cm(OR,1.84;95%CI,1.17-2.87;p=0.009)和分级 III-IV(OR,7.90;95%CI,1.79-34.90;p=0.006)是 LNM 的独立危险因素。根据 OR 值,LNM 的风险评分如下:位于胰体/尾部的肿瘤评分为 1,位于胰头部的肿瘤评分为 4;肿瘤<1cm 评分为 1,≥1.5-2cm 评分为 2;肿瘤分级 I-II 评分为 1,分级 III-IV 评分为 8。最后,该队列的中位数评分为 4,四分位距为 3-6。因此,根据风险评分系统,患者被分为三组:低危组总分为 1-3 分,中危组 4-6 分(OR,2.98;95%CI,1.59-5.60;p=0.001),高危组 7-14 分(OR,8.94;95%CI,4.50-17.7;p<0.001),LNM 发生率分别为 5.0%、13.5%和 31.8%(p<0.001)。
对于有 LNM 恶性潜能的小 NF-PNETs,建议行手术切除伴区域淋巴结清扫术。基于肿瘤分级、位置和大小的 LNM 风险评分可在术前预测小 NF-PNETs 的 LNM,并指导临床实践。