Department of Pancreatic Surgery, Fudan University Shanghai Cancer Center, 270 DongAn Road, Shanghai, 200032, People's Republic of China.
Department of Oncology, Shanghai Medical College, Fudan University, Shanghai, People's Republic of China.
BMC Surg. 2022 May 10;22(1):160. doi: 10.1186/s12893-022-01595-y.
Although some factors that predict the prognosis in pancreatic neuroendocrine tumor (pNET) have been confirmed, the predictive value of lymph node metastasis (LNM) in the prognosis of pNETs remains conflicting and it is not clear whether regional lymphadenectomy should be performed in all grades of tumors.
We included pNET patients undergoing surgery in Shanghai pancreatic cancer institute (SHPCI). The risk factors for survival were investigated by the Kaplan-Meier method and Cox regression model. We evaluated the predictors of LNM using Logistic regression.
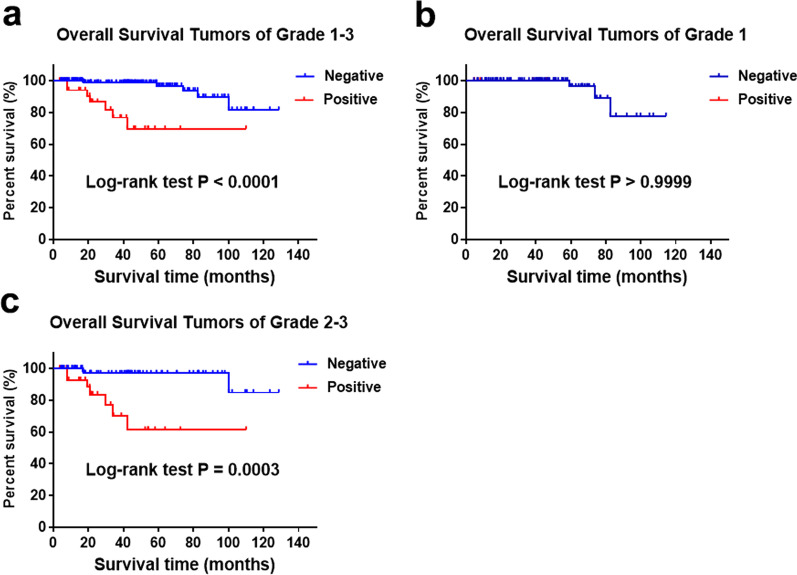
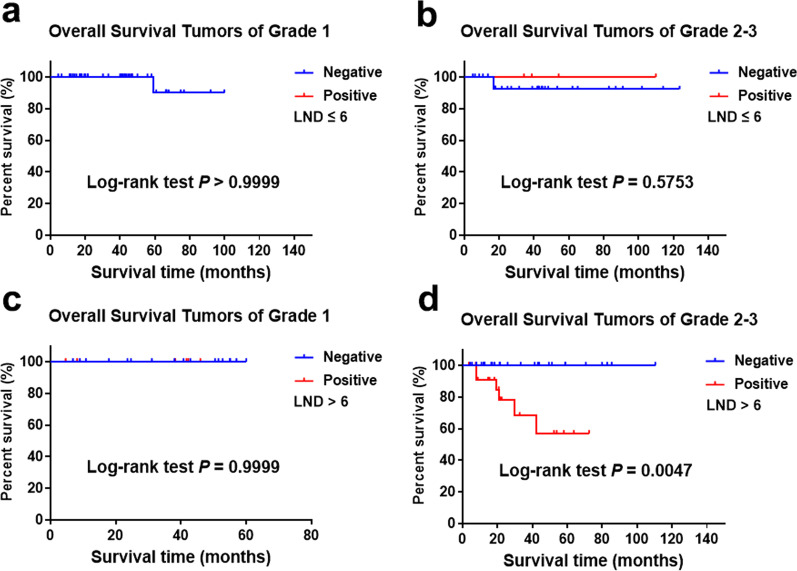
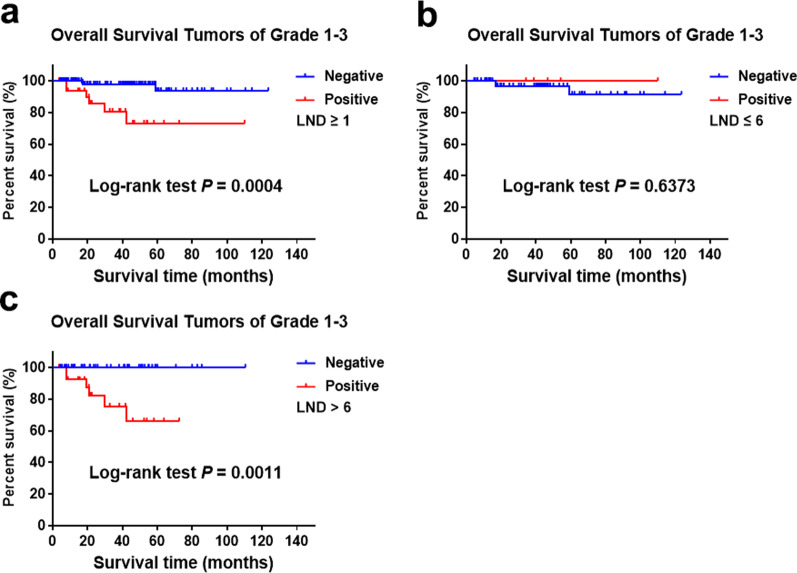
For 206 patients in the SHPCI series, LNM was an independent prognostic factor for entire cohort suggested by multivariate Cox regression analysis. LNM (P = 0.002) predicted poorer overall survival (OS) in grade 2/3 cohort, but there is no significant association between LNM and OS in grade 1 cohort. Grade (P < 0.001) and size (P = 0.049) predicted LNM in entire cohort. Grade (P = 0.002) predicted LNM while regardless of size in grade 2/3 cohort.
Based on our own retrospective data obtained from a single center series, LNM seems to be associated with poorer outcome for patients with grade 2/3 and/or grade 1 > 4 cm tumors. On the other way, LNM was seems to be not associated with prognosis in patients with grade 1 tumors less than 4 cm. Moreover, tumor grade and tumor size seem to act as independent predictors of LNM. Thus, regional lymphadenectomy should be performed in grade 2/3 patients but was not mandatory in grade 1 tumors < 4 cm. It is reasonable to perform functional sparing surgery for grade 1 patients or propose a clinical-radiological monitoring.
虽然已经确定了一些预测胰腺神经内分泌肿瘤(pNET)预后的因素,但淋巴结转移(LNM)在 pNET 预后中的预测价值仍存在争议,也不清楚是否应该对所有分级的肿瘤进行区域淋巴结清扫。
我们纳入了在上海胰腺肿瘤研究所(SHPCI)接受手术的 pNET 患者。采用 Kaplan-Meier 方法和 Cox 回归模型分析生存的危险因素。我们使用 Logistic 回归评估 LNM 的预测因素。
在 SHPCI 系列的 206 名患者中,多变量 Cox 回归分析显示 LNM 是整个队列的独立预后因素。LNM(P=0.002)预测 2/3 级队列的总生存期(OS)较差,但在 1 级队列中,LNM 与 OS 之间无显著相关性。分级(P<0.001)和大小(P=0.049)预测整个队列中的 LNM。分级(P=0.002)预测 2/3 级队列中的 LNM,而与大小无关。
基于我们从单中心系列获得的自身回顾性数据,LNM 似乎与 2/3 级和/或 1 级>4cm 肿瘤患者的预后较差相关。另一方面,LNM 似乎与 1 级肿瘤<4cm 的患者的预后无关。此外,肿瘤分级和肿瘤大小似乎是 LNM 的独立预测因素。因此,区域淋巴结清扫应在 2/3 级患者中进行,但在 1 级肿瘤<4cm 时并非强制性。对 1 级患者进行功能保留手术或提出临床-影像学监测是合理的。