Kawai Keita, Iwamoto Kunihiro, Miyata Seiko, Okada Ippei, Ando Motoo, Fujishiro Hiroshige, Noda Akiko, Ozaki Norio
Department of Psychiatry, Nagoya University Graduate School of Medicine, Nagoya, Japan.
Department of Biomedical Sciences, Chubu University Graduate School of Life and Health Sciences, Kasugai, Japan.
Nat Sci Sleep. 2022 Jul 15;14:1273-1283. doi: 10.2147/NSS.S366774. eCollection 2022.
Sleep state misperception, which is the discrepancy between subjective and objective sleep, is often observed in patients with depression. This phenomenon may delay the remission of depression. Previous studies have focused on the total sleep time (TST) misperception, with many of these studies using actigraphy. Thus, our study investigated depressed patients with the exploratory aim of clarifying factors associated with the sleep state misperception including the wake after sleep onset (WASO) misperception, with their objective sleep additionally evaluated by polysomnography (PSG).
We conducted a cross-sectional study. Before undergoing overnight PSG monitoring, 40 patients with depression completed questionnaires that included the Beck Depression Inventory (BDI), Epworth sleepiness scale, Temperament and Character Inventory, and the Pittsburgh sleep quality index. Patients were also asked to estimate their subjective sleep duration after they woke up in the morning. Based on this data, we calculated the misperception using the following formula: subjective sleep duration minus objective sleep duration. We compared each factor between negative and positive misperception groups and the multiple regression analysis was performed for TST and WASO misperception, respectively.
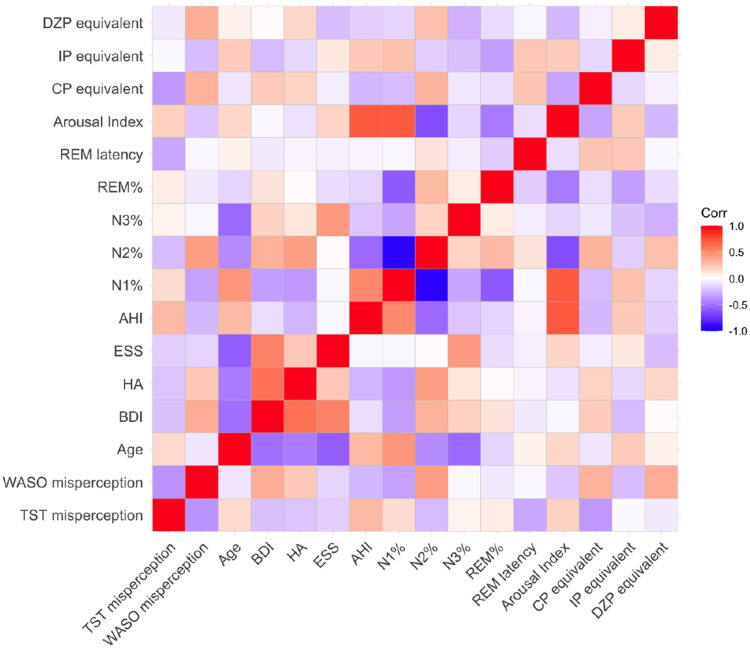
Although sleep architectures, age, severity of depression and obstructive sleep apnea (OSA) exhibited differences in underestimating or overestimating the WASO, only sex differences were associated with underestimating or overestimating their total sleep time (TST). Moreover, BDI, the severity of OSA, sleep architectures (N1% and N2%), and benzodiazepine (BZD) use were significantly correlated with WASO misperception, whereas only OSA severity was significantly correlated with TST misperception. A subsequent multiple regression analysis demonstrated the BDI was independently correlated with the WASO misperception (β=0.341, =0.049).
In clinical practice, interventions especially for OSA, and the reduction of depressive symptoms are an important method for improving patient sleep perception. Moreover, current results suggest that BZD prescriptions should be avoided as well.
睡眠状态误判,即主观睡眠与客观睡眠之间的差异,在抑郁症患者中经常被观察到。这种现象可能会延迟抑郁症的缓解。先前的研究主要集中在总睡眠时间(TST)误判上,其中许多研究使用了活动记录仪。因此,我们的研究以探索性目的调查了抑郁症患者,以阐明与睡眠状态误判相关的因素,包括睡眠起始后觉醒(WASO)误判,并通过多导睡眠图(PSG)对他们的客观睡眠进行额外评估。
我们进行了一项横断面研究。在接受夜间PSG监测之前,40名抑郁症患者完成了问卷,包括贝克抑郁量表(BDI)、爱泼华嗜睡量表、气质和性格量表以及匹兹堡睡眠质量指数。患者还被要求在早上醒来后估计他们的主观睡眠时间。基于这些数据,我们使用以下公式计算误判:主观睡眠时间减去客观睡眠时间。我们比较了阴性和阳性误判组之间的每个因素,并分别对TST和WASO误判进行了多元回归分析。
尽管睡眠结构、年龄、抑郁严重程度和阻塞性睡眠呼吸暂停(OSA)在低估或高估WASO方面存在差异,但只有性别差异与低估或高估他们的总睡眠时间(TST)有关。此外,BDI、OSA严重程度、睡眠结构(N1%和N2%)以及苯二氮䓬(BZD)的使用与WASO误判显著相关,而只有OSA严重程度与TST误判显著相关。随后的多元回归分析表明BDI与WASO误判独立相关(β=0.341,P=0.049)。
在临床实践中,特别是针对OSA的干预措施以及减轻抑郁症状是改善患者睡眠感知的重要方法。此外,目前的结果表明也应避免开具BZD处方。