Kumar Pankaj, Kumar Sanjeev, Hussain Mumtaz, Singh Ritu, Ahmed Waquas, Anand Ravi
Department of Anaesthesiology, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India.
Department of Critical Care Medicine, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India.
Indian J Anaesth. 2022 Jun;66(Suppl 4):S207-S212. doi: 10.4103/ija.ija_41_22. Epub 2022 Jun 6.
Percutaneous dilational tracheostomy (PDT) is a common procedure in intensive care unit (ICU) patients requiring long-term mechanical ventilation. PDT has gradually replaced surgical tracheostomy because it is associated with minimal invasiveness, reduced bleeding and simplicity in technique.This study was conducted to compare ultrasound-guided PDT versus conventional tracheostomy in terms of duration of the procedure, number of passes and immediate peri-procedural complications.
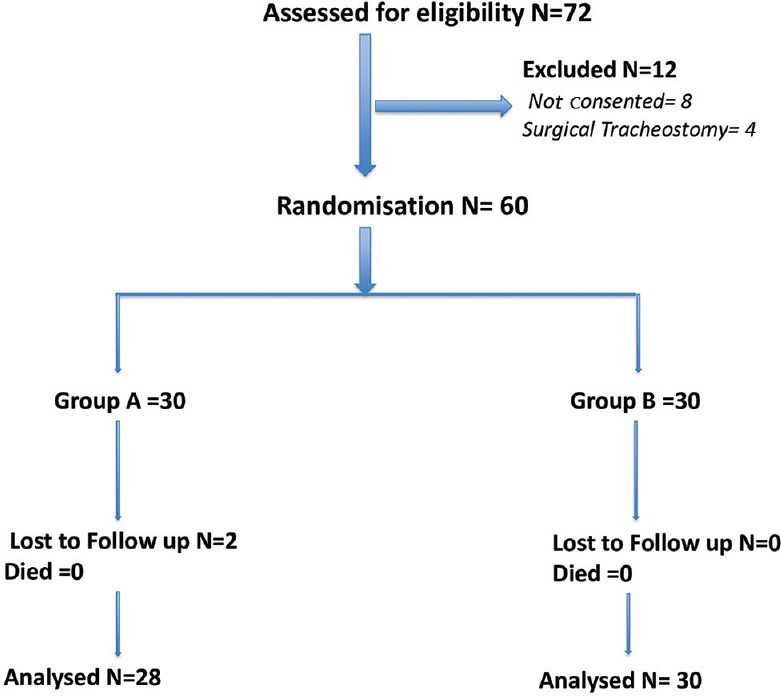
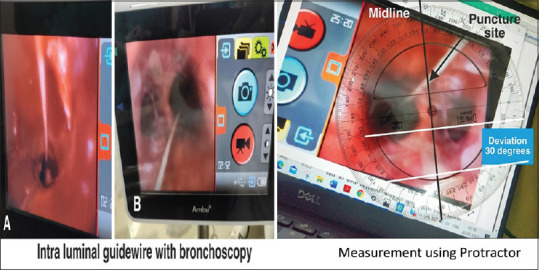
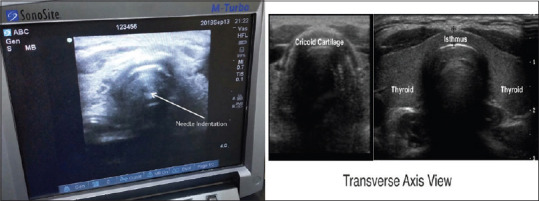
A total of 72 patients with clinical indications of tracheostomy were recruited. A total of 12 patients met the exclusion criteria. The remaining were randomly assigned into two groups of 30 each: Group A (Landmark) with traditional anatomical landmark and Group B (USG) with real-time ultrasound guidance. Puncture positions were recorded with bronchoscopy. Midline deviation was captured on a bronchoscopy image using a protractor. Data on procedural safety and efficacy were also collected.
Group B had significantly fewer cases of midline deviation (11.33 ± 9.51) in comparison to Group A (16.60 ± 12.31). Trials > 2 were equal to 11 in Group A and 2 in Group B. However, the duration of the procedure was higher in Group B (20.07 ± 3.25 min) as compared to Group A (15.20 ± 3.71 min). Peri-procedural and post-procedural complications were also higher in the Landmark group.
Ultrasound-guided PDT showed superiority over landmark PDT in terms of less number of trials, midline puncture and fewer complications. However, it took a little longer to perform USG-guided PDT.
经皮扩张气管切开术(PDT)是重症监护病房(ICU)中需要长期机械通气患者的常见手术。PDT 已逐渐取代外科气管切开术,因为它具有微创性、出血少和技术简单的特点。本研究旨在比较超声引导下的 PDT 与传统气管切开术在手术时间、穿刺次数和围手术期即刻并发症方面的差异。
共招募了 72 例有气管切开临床指征的患者。共有 12 例患者符合排除标准。其余患者随机分为两组,每组 30 例:A 组(地标法)采用传统解剖标志,B 组(超声引导组)采用实时超声引导。用支气管镜记录穿刺位置。使用量角器在支气管镜图像上测量中线偏差。还收集了手术安全性和有效性的数据。
与 A 组(16.60±12.31)相比,B 组中线偏差病例明显更少(11.33±9.51)。A 组穿刺次数>2 次的有 11 例,B 组为 2 例。然而,B 组的手术时间(20.07±3.25 分钟)高于 A 组(15.20±3.71 分钟)。地标法组的围手术期和术后并发症也更高。
超声引导下的 PDT 在穿刺次数、中线穿刺和并发症较少方面显示出优于地标法 PDT 的优势。然而,超声引导下的 PDT 手术时间稍长。