Department of Microbiology, Immunology and Physiology, Meharry Medical College, Nashville, TN, United States.
Arkana Laboratories, Little Rock, AR, United States.
Front Immunol. 2022 Jul 7;13:952235. doi: 10.3389/fimmu.2022.952235. eCollection 2022.
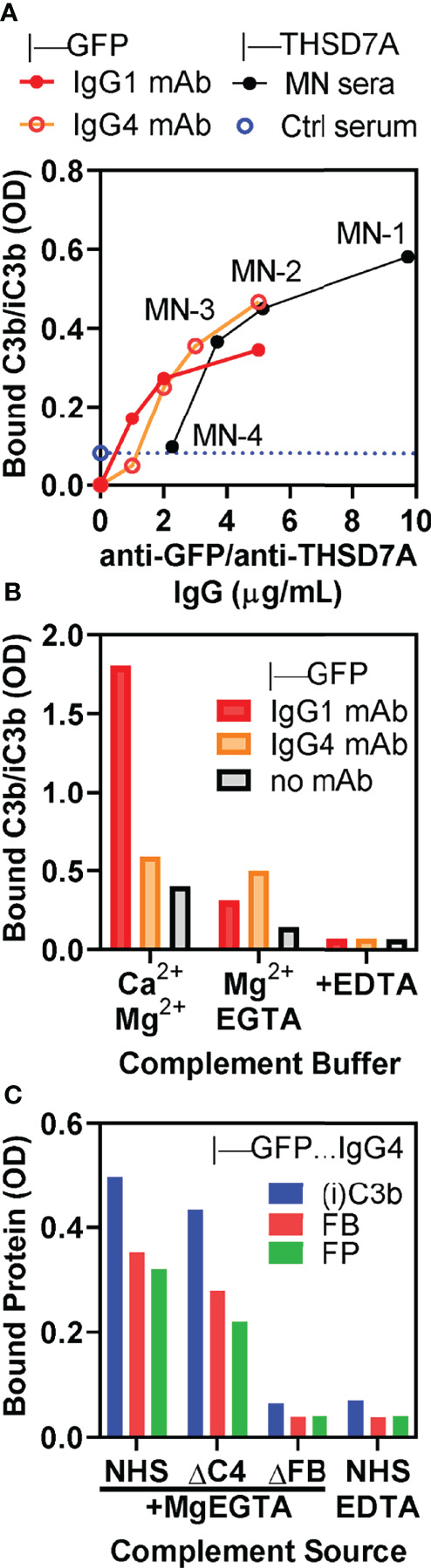
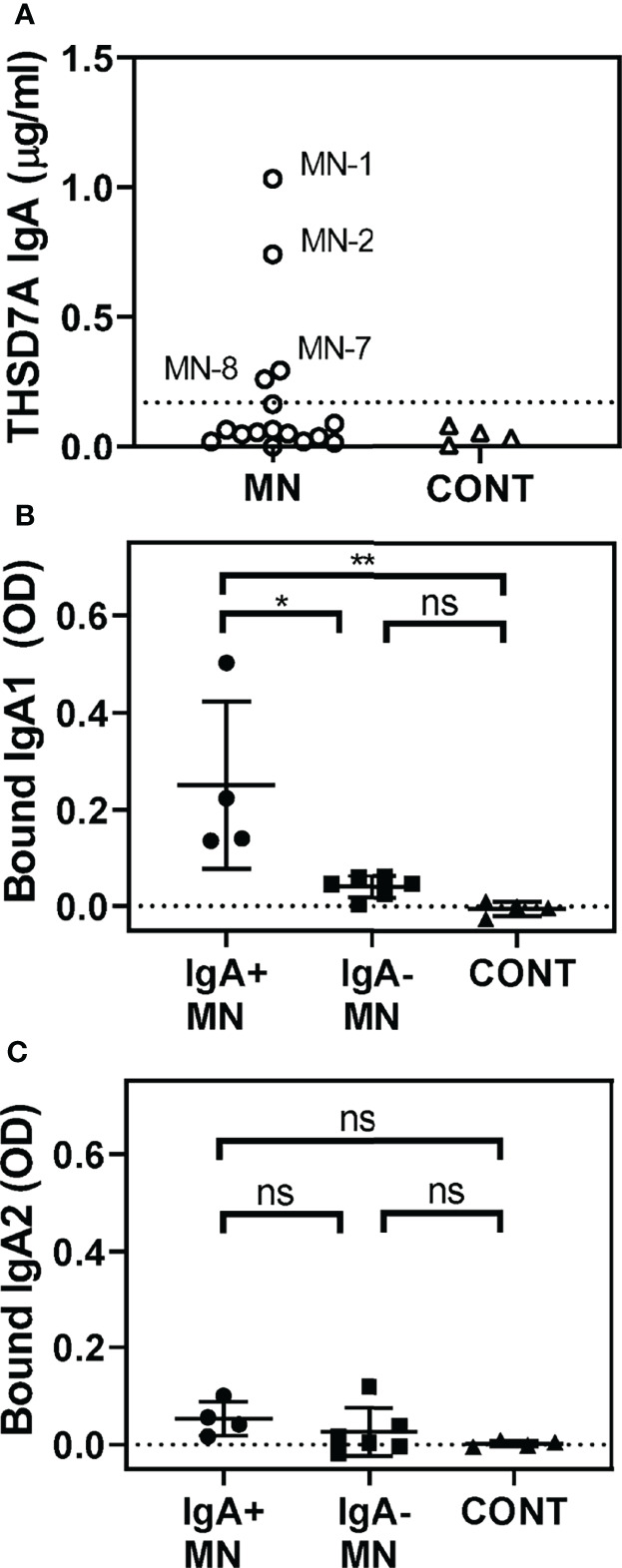
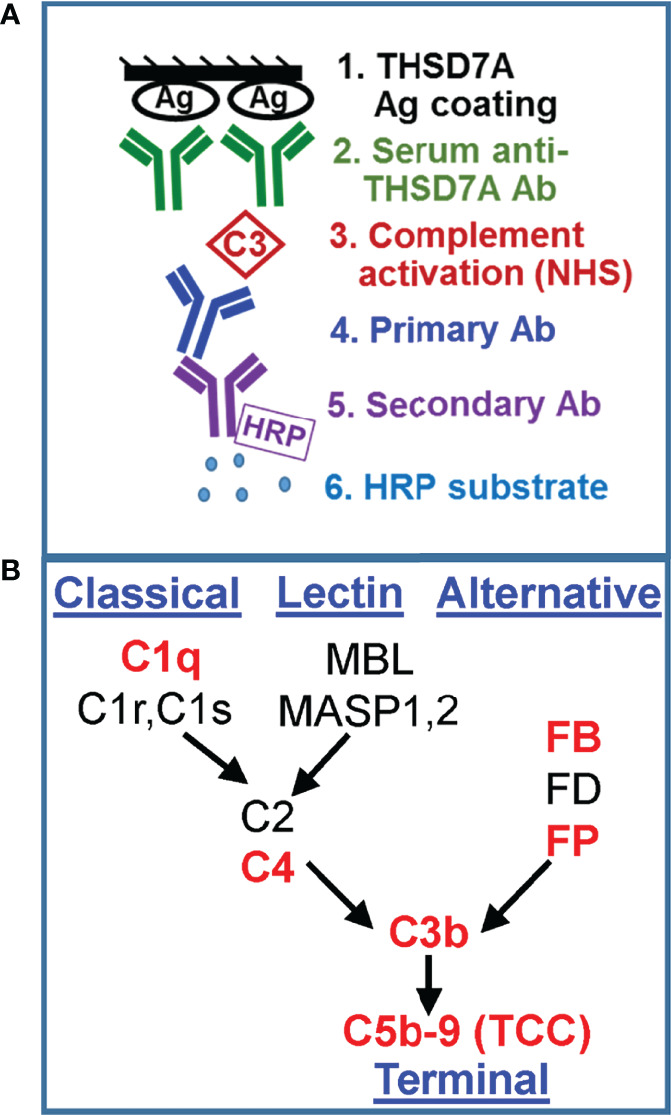
Membranous nephropathy (MN) is an immune kidney disease characterized by glomerular subepithelial immune complexes (ICs) containing antigen, IgG, and products of complement activation. Whereas proteinuria is caused by complement-mediated podocyte injury, the pathways of complement activation remain controversial due to the predominance of IgG4 in ICs, an IgG subclass considered unable to activate complement. THSD7A, a transmembrane protein expressed on podocytes, is the target autoantigen in ~3% of cases of primary MN. In this study, we analyzed sera from 16 patients with THSD7A-associated MN with regard to the anti-THSD7A IgG subclasses and their ability to fix complement . The serum concentration of anti-THSD7A IgG varied over two orders of magnitude (1.3-243 μg/mL). As a relative proportion of all IgG anti-THSD7A, IgG4 was by far the most abundant subclass (median 79%), followed by IgG1 (median 11%). IgG4 was the dominant subclass of anti-THSD7A antibodies in 14 sera, while IgG1 was dominant in one and co-dominant in another. One quarter of MN sera additionally contained low levels of anti-THSD7A IgA1. ICs formed by predominantly IgG4 anti-THSD7A autoantibodies with immobilized THSD7A were relatively weak activators of complement , compared to human IgG1 and IgG3 mAbs used as positive control. Complement deposition on THSD7A ICs was dose-dependent and occurred to a significant extent only at relatively high concentration of anti-THSD7A IgG. C3b fixation by THSD7A ICs was completely abolished in factor B-depleted sera, partially inhibited in C4-depleted sera, unchanged in C1q-depleted sera, and also occurred in Mg-EGTA buffer. These results imply that THSD7A ICs predominantly containing IgG4 activate complement at high IgG4 density, which strictly requires a functional alternative pathway, whereas the classical and lectin pathways are dispensable. These findings advance our understanding of how IgG4 antibodies activate complement.
膜性肾病 (MN) 是一种免疫性肾脏疾病,其特征是肾小球上皮下免疫复合物 (IC) 中含有抗原、IgG 和补体激活产物。虽然蛋白尿是由补体介导的足细胞损伤引起的,但由于 IC 中 IgG4 占优势,补体激活途径仍存在争议,因为 IgG4 被认为不能激活补体。THSD7A 是一种表达在足细胞上的跨膜蛋白,是约 3%的原发性 MN 病例的自身抗原靶标。在这项研究中,我们分析了 16 例 THSD7A 相关 MN 患者的血清,研究了抗 THSD7A IgG 亚类及其补体固定能力。抗 THSD7A IgG 的血清浓度跨越了两个数量级(1.3-243μg/ml)。作为所有 IgG 抗 THSD7A 的相对比例,IgG4 是迄今为止最丰富的亚类(中位数 79%),其次是 IgG1(中位数 11%)。在 14 份血清中,IgG4 是抗 THSD7A 抗体的主要亚类,而在 1 份血清中 IgG1 是主要亚类,在另 1 份血清中是共同主导亚类。四分之一的 MN 血清还含有低水平的抗 THSD7A IgA1。与作为阳性对照的人 IgG1 和 IgG3 mAb 相比,主要由 IgG4 抗 THSD7A 自身抗体形成的 IC 对补体的激活作用相对较弱。THSD7A IC 上的补体沉积呈剂量依赖性,仅在相对较高浓度的抗 THSD7A IgG 时才会显著发生。在耗尽因子 B 的血清中,THSD7A IC 上的 C3b 固定完全被阻断,在耗尽 C4 的血清中部分被抑制,在耗尽 C1q 的血清中未改变,在 Mg-EGTA 缓冲液中也会发生。这些结果表明,主要含有 IgG4 的 THSD7A IC 在高 IgG4 密度下激活补体,这严格需要一个功能替代途径,而经典途径和凝集素途径是可有可无的。这些发现加深了我们对 IgG4 抗体如何激活补体的理解。