Department of Rehabilitation Sciences, KU Leuven-University of Leuven, Leuven, Belgium.
Department of Abdominal Surgery, University Hospitals Gasthuisberg Leuven and KU Leuven-University of Leuven, Leuven, Belgium.
Ann Surg. 2022 Nov 1;276(5):761-768. doi: 10.1097/SLA.0000000000005632. Epub 2022 Jul 27.
Total mesorectal excision (TME) for rectal cancer (RC) often results in significant bowel symptoms, commonly known as low anterior resection syndrome (LARS). Although pelvic floor muscle training (PFMT) is recommended in noncancer populations for treating bowel symptoms, this has been scarcely investigated in RC patients. The objective was to investigate PFMT effectiveness on LARS in patients after TME for RC.
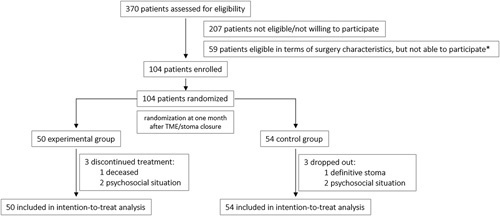
A multicenter, single-blind prospective randomized controlled trial comparing PFMT (intervention; n=50) versus no PFMT (control; n=54) 1 month following TME/stoma closure was performed. The primary endpoint was the proportion of participants with an improvement in the LARS category at 4 months. Secondary outcomes were: continuous LARS scores, ColoRectal Functioning Outcome scores, Numeric Rating Scale scores, stool diary items, and Short Form 12 scores; all assessed at 1, 4, 6, and 12 months.
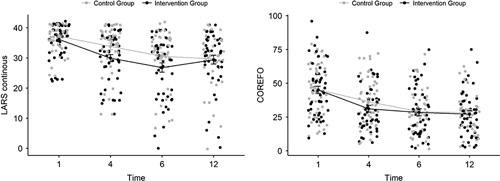
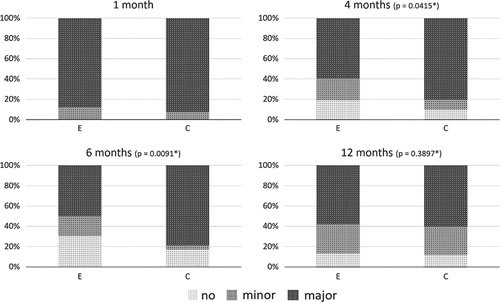
The proportion of participants with an improvement in LARS category was statistically higher after PFMT compared with controls at 4 months (38.3% vs 19.6%; P =0.0415) and 6 months (47.8% vs 21.3%; P =0.0091), but no longer at 12 months (40.0% vs 34.9%; P =0.3897). Following secondary outcomes were significantly lower at 4 months: LARS scores (continuous, P =0.0496), ColoRectal Functioning Outcome scores ( P =0.0369) and frequency of bowel movements ( P =0.0277), solid stool leakage (day, P =0.0241; night, P =0.0496) and the number of clusters ( P =0.0369), derived from the stool diary. No significant differences were found for the Numeric Rating Scale/quality of life scores.
PFMT for bowel symptoms after TME resulted in lower proportions and faster recovery of bowel symptoms up to 6 months after surgery/stoma closure, justifying PFMT as an early, first-line treatment option for bowel symptoms after RC.
直肠癌(RC)的全直肠系膜切除术(TME)常导致明显的肠道症状,通常称为低位前切除综合征(LARS)。尽管盆腔底肌肉训练(PFMT)在非癌症人群中被推荐用于治疗肠道症状,但在 RC 患者中对此研究甚少。本研究旨在探讨 TME 后 RC 患者接受 PFMT 对 LARS 的影响。
进行了一项多中心、单盲前瞻性随机对照试验,比较了 TME/造口关闭后 1 个月时接受 PFMT(干预组,n=50)与不接受 PFMT(对照组,n=54)的患者,主要终点是 4 个月时 LARS 类别的改善比例。次要结局为:连续 LARS 评分、ColoRectal Functioning Outcome 评分、数字评分量表评分、粪便日记项目和健康调查简表 12 项(SF-12)评分,所有评分均在 1、4、6 和 12 个月时进行评估。
与对照组相比,PFMT 组在 4 个月(38.3%比 19.6%;P=0.0415)和 6 个月(47.8%比 21.3%;P=0.0091)时 LARS 类别的改善比例更高,而在 12 个月时则无统计学差异(40.0%比 34.9%;P=0.3897)。次要结局在 4 个月时明显更低:LARS 评分(连续,P=0.0496)、ColoRectal Functioning Outcome 评分(P=0.0369)和排便频率(P=0.0277),粪便日记中固体粪便漏出(白天,P=0.0241;晚上,P=0.0496)和粪便群数(P=0.0369)。数字评分量表/生活质量评分无显著差异。
TME 后进行 PFMT 治疗可使肠道症状的比例更低,且术后/造口关闭后 6 个月内更快恢复,这证明 PFMT 是 RC 后肠道症状的早期一线治疗选择。