New Balance Foundation Obesity Prevention Center, Boston Children's Hospital, Boston, MA, USA.
Department of Pediatrics, Harvard Medical School, Boston, MA, USA.
Eur J Clin Nutr. 2022 Sep;76(9):1209-1221. doi: 10.1038/s41430-022-01179-2. Epub 2022 Jul 28.
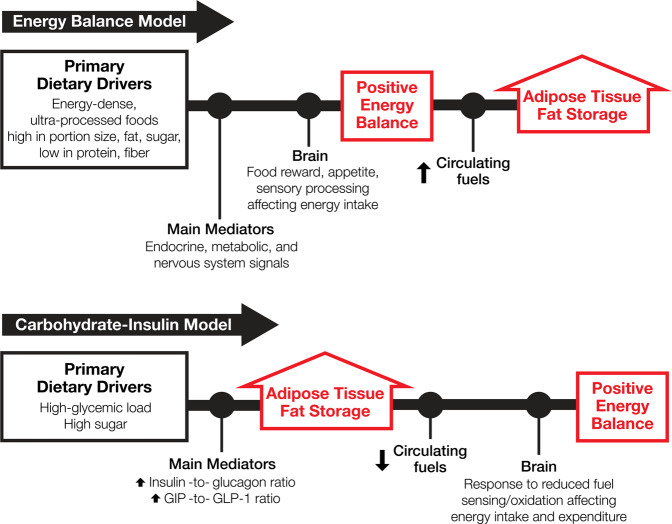
The obesity pandemic continues unabated despite a persistent public health campaign to decrease energy intake ("eat less") and increase energy expenditure ("move more"). One explanation for this failure is that the current approach, based on the notion of energy balance, has not been adequately embraced by the public. Another possibility is that this approach rests on an erroneous paradigm. A new formulation of the energy balance model (EBM), like prior versions, considers overeating (energy intake > expenditure) the primary cause of obesity, incorporating an emphasis on "complex endocrine, metabolic, and nervous system signals" that control food intake below conscious level. This model attributes rising obesity prevalence to inexpensive, convenient, energy-dense, "ultra-processed" foods high in fat and sugar. An alternative view, the carbohydrate-insulin model (CIM), proposes that hormonal responses to highly processed carbohydrates shift energy partitioning toward deposition in adipose tissue, leaving fewer calories available for the body's metabolic needs. Thus, increasing adiposity causes overeating to compensate for the sequestered calories. Here, we highlight robust contrasts in how the EBM and CIM view obesity pathophysiology and consider deficiencies in the EBM that impede paradigm testing and refinement. Rectifying these deficiencies should assume priority, as a constructive paradigm clash is needed to resolve long-standing scientific controversies and inform the design of new models to guide prevention and treatment. Nevertheless, public health action need not await resolution of this debate, as both models target processed carbohydrates as major drivers of obesity.
尽管公众健康运动一直在持续,旨在减少能量摄入(“少吃”)和增加能量消耗(“多运动”),但肥胖大流行仍在继续。这种方法未能取得成功的一个解释是,当前基于能量平衡概念的方法并没有被公众充分接受。另一种可能性是,这种方法基于错误的范式。与之前的版本一样,新的能量平衡模型(EBM)考虑到过量进食(能量摄入>支出)是肥胖的主要原因,强调了控制无意识下食物摄入的“复杂内分泌、代谢和神经系统信号”。该模型将肥胖患病率的上升归因于便宜、方便、能量密集、高脂肪和高糖的“超加工”食品。另一种观点,即碳水化合物-胰岛素模型(CIM),则提出对高度加工碳水化合物的激素反应会将能量分配转向脂肪组织的沉积,从而减少可供身体代谢需求的卡路里。因此,增加肥胖会导致过量进食以补偿被隔离的卡路里。在这里,我们重点强调了 EBM 和 CIM 对肥胖病理生理学的看法之间的明显对比,并考虑了 EBM 的缺陷,这些缺陷阻碍了范式的测试和改进。纠正这些缺陷应该是优先事项,因为建设性的范式冲突需要解决长期存在的科学争议,并为预防和治疗提供新的模型设计。然而,公共卫生行动不必等待这场辩论的解决,因为这两种模型都将加工碳水化合物作为肥胖的主要驱动因素。