Traver Edward C, Heil Emily L, Schmalzle Sarah A
Division of Infectious Disease, Department of Medicine, University of Maryland School of Medicine, Baltimore, Maryland, USA.
Department of Pharmacy Practice and Science, University of Maryland School of Pharmacy, Baltimore, Maryland, USA.
Open Forum Infect Dis. 2022 Jul 1;9(7):ofac331. doi: 10.1093/ofid/ofac331. eCollection 2022 Jul.
Serotonin toxicity (also referred to as serotonin syndrome) results from medications that affect the neurotransmitter serotonin. The antibiotic linezolid and the opioids methadone and buprenorphine are all reported to cause serotonin toxicity, but the degree of risk with use of linezolid in combination with methadone or buprenorphine is unknown.
We conducted a retrospective cross-sectional analysis of adult patients hospitalized from November 2015 to October 2019 who were administered linezolid in combination with methadone and/or buprenorphine within 24 hours and a subgroup that received the combination for ≥3 days. Cases of serotonin toxicity were identified from the clinical notes in the electronic medical record and were classified as possible or definite based on the clinical record. The Hunter diagnostic criteria were retrospectively applied.
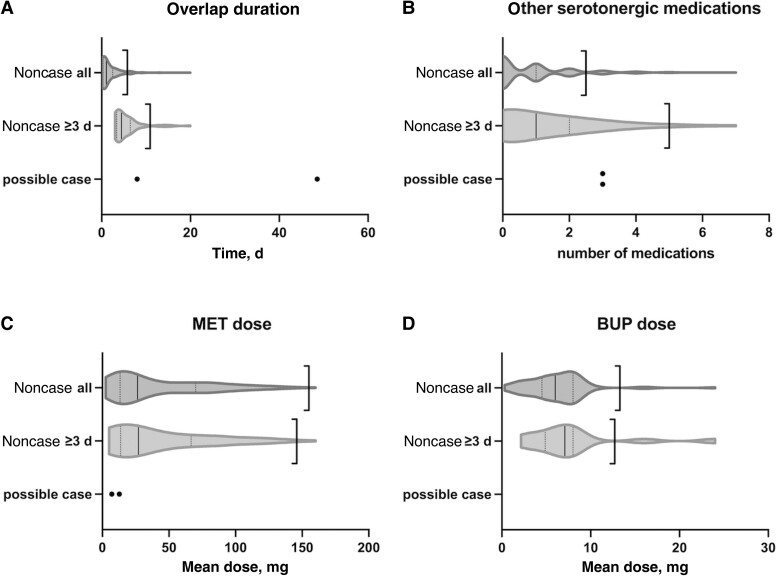
There were 494 encounters in which linezolid was administered concurrently with methadone and buprenorphine. The mean patient age was 42.5 years, and 52.4% of encounters were of female patients. The mean duration of concurrent administration was 1.9 days. There were 106 encounters with a duration of concurrent administration ≥3 days (mean, 5.4 days). Two cases of possible serotonin toxicity and 0 cases of definite serotonin toxicity occurred; neither possible case met the Hunter criteria from the available information. Possible cases occurred in 0.40% of all encounters and 1.89% of encounters with ≥3 days of overlap (upper 1-sided 95% CI, 0.87% and 4.06%).
Serotonin toxicity occurring during the administration of linezolid in combination with methadone and/or buprenorphine occurred rarely among 494 hospital encounters, including 106 encounters with ≥3 days of overlap. Limitations include potential missed diagnoses of serotonin toxicity and short durations of overlap. Further study evaluating the short-term risk of this combination is needed.
血清素毒性(也称为血清素综合征)由影响神经递质血清素的药物引起。据报道,抗生素利奈唑胺以及阿片类药物美沙酮和丁丙诺啡都会导致血清素毒性,但利奈唑胺与美沙酮或丁丙诺啡联合使用时的风险程度尚不清楚。
我们对2015年11月至2019年10月期间住院的成年患者进行了一项回顾性横断面分析,这些患者在24小时内接受了利奈唑胺与美沙酮和/或丁丙诺啡的联合治疗,以及一个接受联合治疗≥3天的亚组。从电子病历的临床记录中识别出血清素毒性病例,并根据临床记录将其分类为可能或确定病例。回顾性应用亨特诊断标准。
有494次利奈唑胺与美沙酮和丁丙诺啡同时给药的情况。患者的平均年龄为42.5岁,52.4%的情况为女性患者。同时给药的平均持续时间为1.9天。有106次同时给药持续时间≥3天(平均5.4天)。发生了2例可能的血清素毒性病例,确定的血清素毒性病例为0例;根据现有信息,这两例可能病例均不符合亨特标准。可能病例在所有情况中占0.40%,在重叠≥3天的情况中占1.89%(单侧95%置信区间上限,0.87%和4.06%)。
在494次住院情况中,包括106次重叠≥3天的情况,利奈唑胺与美沙酮和/或丁丙诺啡联合给药期间发生血清素毒性的情况很少见。局限性包括血清素毒性可能漏诊以及重叠时间短。需要进一步研究评估这种联合用药的短期风险。