Division of Pharmacology and Vascular Medicine, Department of Internal Medicine, Erasmus MC, University Medical Center Rotterdam, the Netherlands (E.O.C.L., D.Y., E.U., A.H.J.D.).
Saha Cardiovascular Research Center (C.W., H.S.L.), University of Kentucky.
Hypertension. 2022 Oct;79(10):2115-2126. doi: 10.1161/HYPERTENSIONAHA.122.18731. Epub 2022 Jul 29.
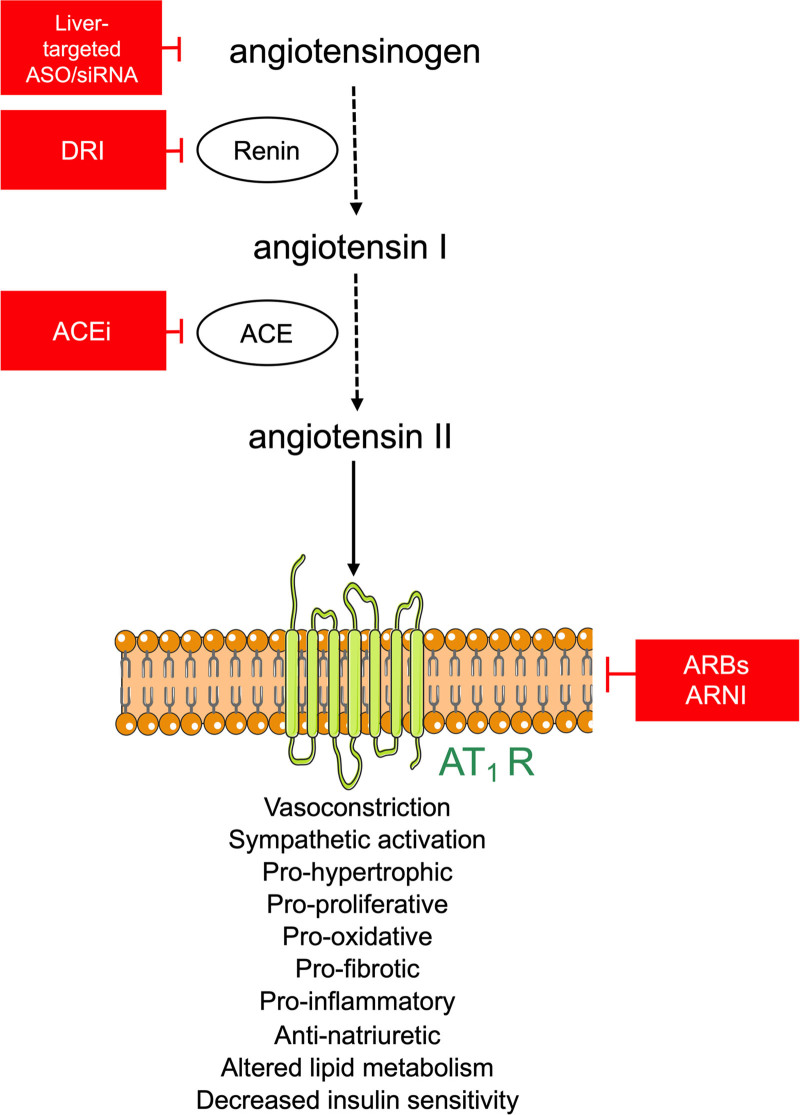
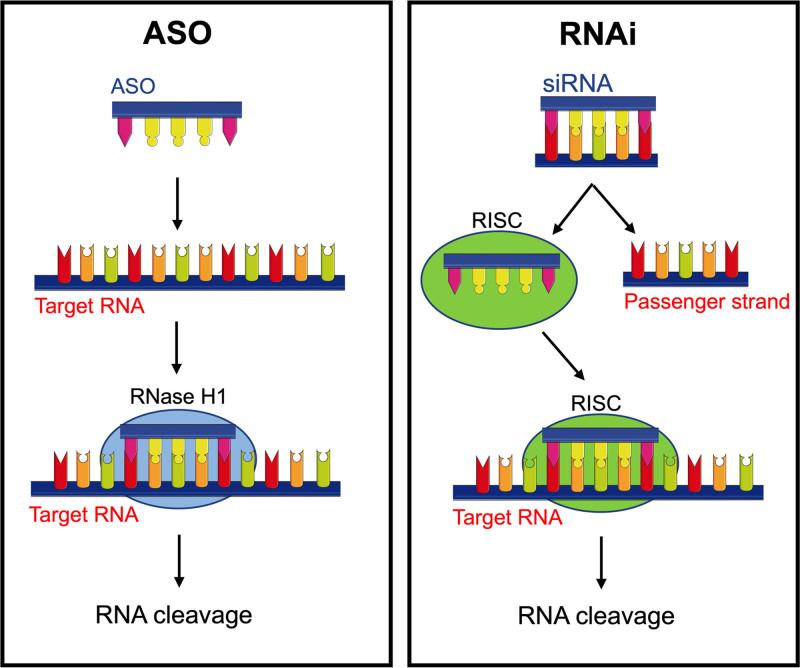
Multiple types of renin-angiotensin system (RAS) blockers exist, allowing interference with the system at the level of renin, angiotensin-converting enzyme, or the angiotensin II receptor. Yet, in particular, for the treatment of hypertension, the number of patients with uncontrolled hypertension continues to rise, either due to patient noncompliance or because of the significant renin rises that may, at least partially, overcome the effect of RAS blockade (RAS escape). New approaches to target the RAS are either direct antisense oligonucleotides that inhibit angiotensinogen RNA translation, or small interfering RNA (siRNA) that function via the RNA interference pathway. Since all angiotensins stem from angiotensinogen, lowering angiotensinogen has the potential to circumvent the RAS escape phenomenon. Moreover, antisense oligonucleotides and small interfering RNA require injections only every few weeks to months, which might reduce noncompliance. Of course, angiotensinogen suppression also poses a threat in situations where the RAS is acutely needed, for instance in women becoming pregnant during treatment, or in cases of emergency, when severe hypotension occurs. This review discusses all preclinical data on angiotensinogen suppression, as well as the limited clinical data that are currently available. It concludes that it is an exciting new tool to target the RAS with high specificity and a low side effect profile. Its long-term action might revolutionize pharmacotherapy, as it could overcome compliance problems. Preclinical and clinical programs are now carefully investigating its efficacy and safety profile, allowing an optimal introduction as a novel drug to treat cardiovascular and renal diseases in due time.
存在多种类型的肾素-血管紧张素系统 (RAS) 阻滞剂,可在肾素、血管紧张素转换酶或血管紧张素 II 受体水平干扰该系统。然而,特别是在高血压的治疗中,未得到控制的高血压患者数量仍在继续上升,这要么是由于患者不遵医嘱,要么是由于可能至少部分克服了 RAS 阻断作用的显著肾素升高(RAS 逃逸)。针对 RAS 的新方法要么是直接反义寡核苷酸,可抑制血管紧张素原 RNA 的翻译,要么是小干扰 RNA (siRNA),通过 RNA 干扰途径发挥作用。由于所有血管紧张素都源自血管紧张素原,因此降低血管紧张素原有可能规避 RAS 逃逸现象。此外,反义寡核苷酸和小干扰 RNA 只需每几周至几个月注射一次,这可能会降低不遵医嘱的情况。当然,在 RAS 急需的情况下,如在治疗期间女性怀孕或发生严重低血压的紧急情况下,血管紧张素原抑制也会带来威胁。这篇综述讨论了血管紧张素原抑制的所有临床前数据,以及目前可用的有限临床数据。它得出的结论是,这是一种具有高特异性和低副作用特征的靶向 RAS 的令人兴奋的新工具。其长期作用可能会彻底改变药物治疗,因为它可以克服依从性问题。目前正在进行临床前和临床项目,以仔细研究其疗效和安全性,以便在适当的时候作为一种治疗心血管和肾脏疾病的新药进行优化引入。