National Centre for Emergency Primary Health Care, NORCE Norwegian Research Centre, Box 22 Nygårdstangen, 5838, Bergen, Norway.
Vennesla Health Care Center, Sentrumsvegen 41, 4700, Vennesla, Norway.
BMC Prim Care. 2022 Jul 30;23(1):191. doi: 10.1186/s12875-022-01799-4.
Primary healthcare in Norway has first-line responsibility for medical emergencies, including traumas and fractures. Normally, patients with suspected fractures are referred to specialist care. However, some municipalities have X-ray facilities and handle minor fractures locally. We investigated patient-reported outcome measures after initial treatment of radiologically diagnosed fractures of the wrist, collarbone, and ankle at a primary healthcare centre in a rural municipality with a large ski resort. The patients' general satisfaction with the treatment was also investigated.
Validated questionnaires were sent to patients with fractures of the wrist or collarbone (Quick DASH-Disability of Arm, Shoulder and Hand) or the ankle (FAOS -The Foot and Ankle Outcome Score). Patients with wrist and collarbone fractures also answered the Quality-of-life questions that are a subscale of the FAOS questionnaire for ankle fractures. Patient satisfaction was measured for all fracture groups. The Quick DASH scale ranges from 0 (no disability at all) to 100 (great disability), while for FAOS a score of 100 indicates no symptoms and 0 indicates extreme disabilities.
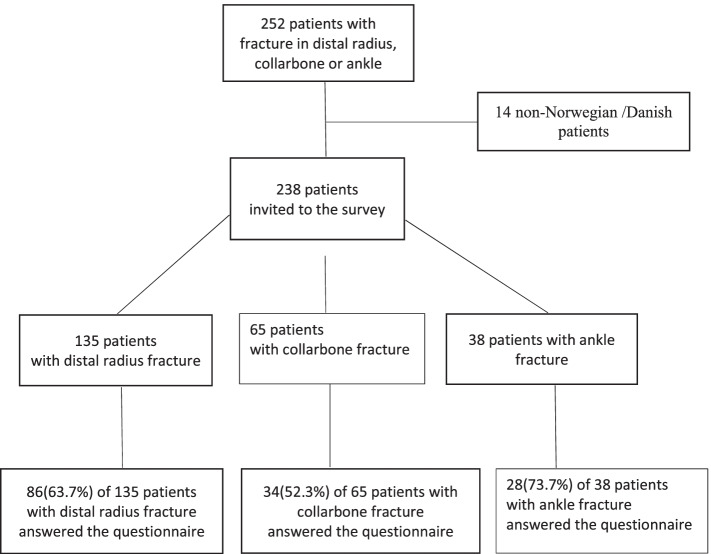
A total of 148 of 238 patients answered the questionnaire (62% response rate). Patients with distal radius fractures had a mean Quick DASH score of 5.1 (median 0, range 0-77), and scores were significantly lower for males (p = 0.013) and increased with age (p = 0.024). Patients with collarbone fractures had a mean Quick DASH score of 2.1 (median 0, range 0-32) with no significant age or gender differences. Patients with ankle fractures had the following mean subscale-scores: Pain, 93.8; Symptoms, 71.4; Activities of daily living, 97.4; Sport, 90.0; and Quality of life, 92.1. The scores did not differ significantly by specialization of the physician. A total of 88% of the patients were highly or very highly satisfied with the handling of their fracture.
The patients reported low rates of functional disability and high rates of satisfaction after initial radiological diagnosis and treatment of their fracture at the primary healthcare centre. Specialisation of the treating physician was not associated with the outcome in any of the fracture types.
挪威的初级医疗保健机构负责处理包括创伤和骨折在内的医疗急症,具有一线责任。通常,疑似骨折的患者会被转介至专科治疗。然而,一些自治市拥有 X 光设施,可以在当地处理轻微骨折。我们调查了在一个拥有大型滑雪胜地的农村自治市的初级保健中心,对放射学诊断的腕部、锁骨和踝关节骨折患者进行初始治疗后的患者报告的结局测量指标,还调查了患者对治疗的总体满意度。
将经过验证的问卷寄给腕部或锁骨骨折(快速残疾量表-上肢、肩部和手)或踝关节骨折(FAOS-足踝结果评分)的患者。腕部和锁骨骨折患者还回答了 FAOS 问卷中踝关节骨折亚量表的生活质量问题。所有骨折组都测量了患者满意度。快速残疾量表的范围为 0(完全无残疾)至 100(严重残疾),而 FAOS 的评分 100 表示无症状,0 表示极度残疾。
238 名患者中有 148 名(62%的回复率)回答了问卷。桡骨远端骨折患者的平均快速残疾量表评分为 5.1(中位数 0,范围 0-77),男性评分显著较低(p=0.013),年龄越大评分越高(p=0.024)。锁骨骨折患者的平均快速残疾量表评分为 2.1(中位数 0,范围 0-32),年龄和性别无显著差异。踝关节骨折患者的以下亚量表评分分别为:疼痛,93.8;症状,71.4;日常生活活动,97.4;运动,90.0;生活质量,92.1。这些评分在医生的专业分工上没有显著差异。总共 88%的患者对他们在初级保健中心骨折的处理非常满意或高度满意。
患者报告在初级保健中心接受放射学诊断和初始治疗后,功能障碍发生率低,对骨折处理的满意度高。在任何一种骨折类型中,治疗医生的专业分工都与结果无关。