Department of Spine Surgery, The First Affiliated Hospital of Xinjiang Medical University, Urumqi, 830054, Xinjiang, China.
Department of Trauma and Microreconstructive Surgery, The First Affiliated Hospital of Xinjiang Medical University, Urumqi, 830054, Xinjiang, China.
BMC Musculoskelet Disord. 2022 Jul 30;23(1):731. doi: 10.1186/s12891-022-05693-z.
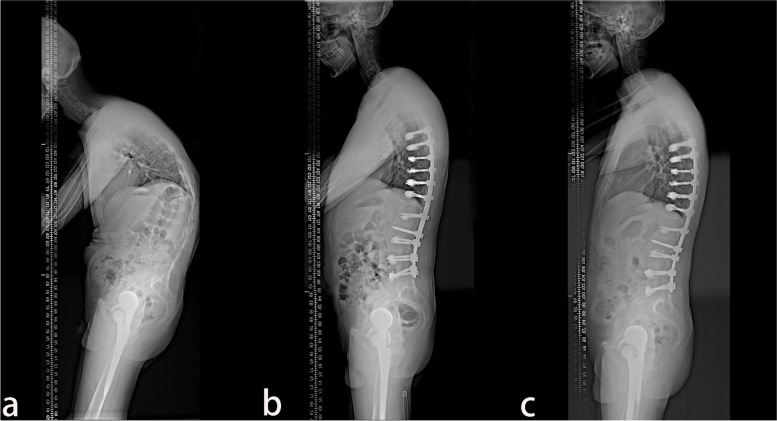
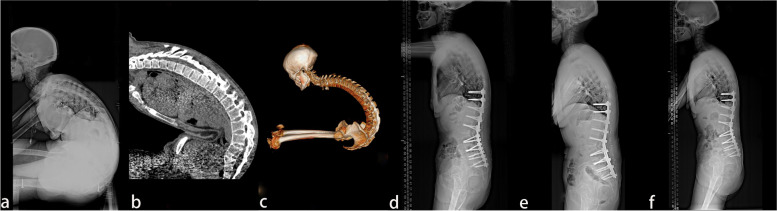
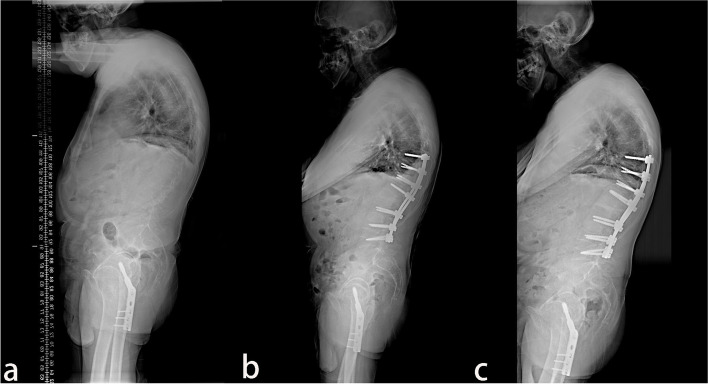
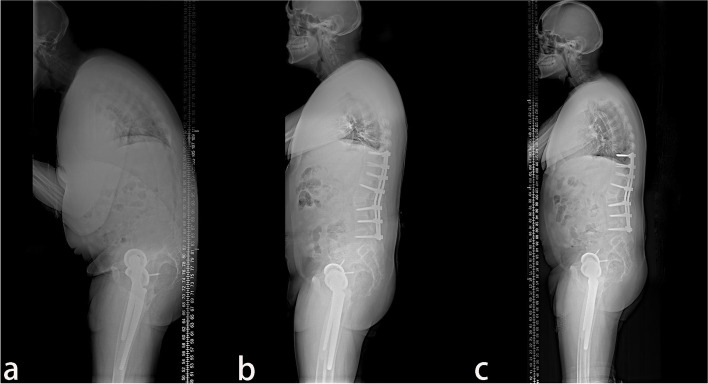
To evaluate the sagittal parameters and clinical outcome of pedicle subtraction osteotomy (PSO) for the treatment of ankylosing spondylitis (AS) combined with thoracolumbar kyphosis.
The clinical data of 38 patients with AS combined with thoracolumbar kyphosis who underwent PSO were enrolled and divided into the lumbar lordosis group and the lumbar kyphosis group according to the preoperative sagittal morphology. They were subdivided into the lumbar lordosis T12 group, lordosis L1 group, kyphosis L2 group, and kyphosis L3 group. The spine sagittal parameters were compared between the preoperative and the postoperative. Outcome evaluation was performed by the Japanese Orthopedic Association (JOA) score, visual analogue scale (VAS), and the Oswestry Disability Index (ODI).
A total of 38 patients with AS combined with thoracolumbar kyphosis were successfully treated by PSO, with a mean follow-up time of 26.9 ± 11.9 months. There were 30 males and 8 females with a mean age of 41.6 ± 7.1 years. Twenty patients consisted in the lumbar lordosis group and 18 patients in the lumbar kyphosis group. GK, SVA, and CBVA were improved significantly (P < 0.05) at the final follow-up between the lumbar lordosis T12 group and the L1 group. Patients in the lumbar kyphosis L2 group and L3 group all received satisfactory, including LL, GK, and SVA (P < 0.05). There was no statistically significant difference in the preoperative TK, GK, SVA, PT, and PI between the lumbar lordosis and lumbar kyphosis groups (P > 0.05). Postoperative complications occurred in three cases.
PSO was a practical method for the treatment of patients with AS combined with thoracolumbar kyphosis. PSO at L3 was recommended to be selected for the lumbar kyphosis to obtain greater SVA correction. CBVA of single-segment PSO may be significantly lower than the two-segment PSO in the management of patients with kyphosis of lower CBVA.
评估经椎弓根截骨术(PSO)治疗强直性脊柱炎(AS)合并胸腰椎后凸畸形的矢状位参数和临床疗效。
回顾性分析 38 例 AS 合并胸腰椎后凸畸形患者行 PSO 的临床资料,根据术前矢状位形态分为腰椎前凸组和腰椎后凸组,再根据术前 T12 段胸腰椎后凸角(TL1)分为腰椎前凸 T12 组、前凸 L1 组、后凸 L2 组和后凸 L3 组。比较患者术前与术后脊柱矢状位参数,采用日本矫形外科学会(JOA)评分、视觉模拟评分(VAS)和 Oswestry 功能障碍指数(ODI)对疗效进行评价。
38 例 AS 合并胸腰椎后凸畸形患者均顺利完成 PSO 治疗,平均随访 26.9±11.9 个月。男 30 例,女 8 例;年龄 22~65 岁,平均 41.6±7.1 岁。腰椎前凸组 20 例,腰椎后凸组 18 例。腰椎前凸 T12 组和前凸 L1 组术后冠状面轴向垂直距离(C7SVA)、骨盆倾斜角(GK)、骨盆入射角(PI)较术前明显改善(P<0.05)。腰椎后凸 L2 组和 L3 组各指标均得到满意矫正,包括矢状面平衡(LL)、GK、SVA(P<0.05)。腰椎前凸组与腰椎后凸组术前胸腰椎后凸角(TK)、PI、SVA、骨盆投射指数(PT)、骨盆倾斜指数(PI)差异均无统计学意义(P>0.05)。术后发生并发症 3 例。
PSO 是治疗 AS 合并胸腰椎后凸畸形的一种有效方法,对于腰椎后凸患者,PSO 于 L3 节段施行更有利于获得较大的 SVA 矫正,对于下颈椎矢状面平衡较差的患者,行单节段 PSO 治疗可能会导致术后矢状面平衡的明显降低。