Katsumata Ryo, Monobe Yasumasa, Akagi Akihisa, Yamatsuji Tomoki, Naomoto Yoshio
Department of Health Care Medicine, Kawasaki Medical School General Medical Center, Okayama, JPN.
Department of Pathology, Kawasaki Medical School General Medical Center, Okayama, JPN.
Cureus. 2022 Jun 29;14(6):e26438. doi: 10.7759/cureus.26438. eCollection 2022 Jun.
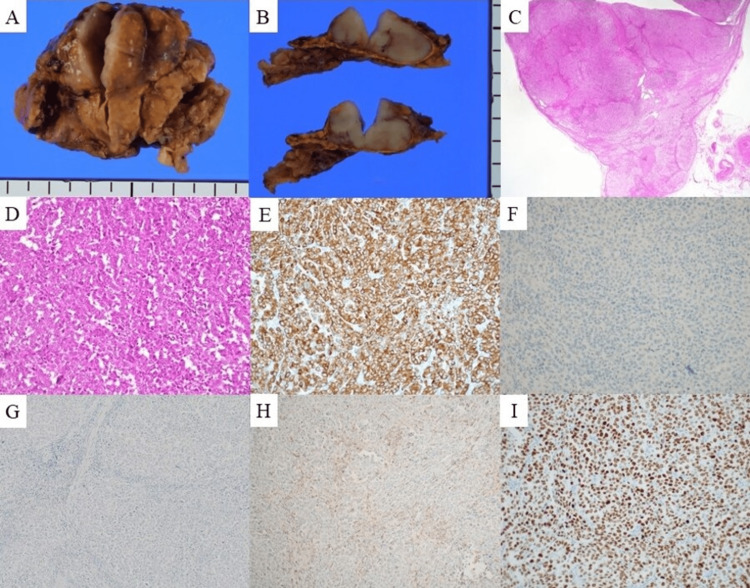
The clinical management of brain metastasis (BM) and adrenal metastasis (AM) of cancer of unknown primary (CUP) can be challenging. A 73-year-old man presented to the hospital with sudden-onset hemiplegia. His laboratory data were normal, except for elevated levels of carcinoembryonic antigen (CEA) (33.8 ng/mL). Contrast-enhanced magnetic resonance imaging revealed a 2-cm mass with ring enhancement in the right parietal lobe and extensive vasogenic edema around the tumor. The lesion was diagnosed as BM; however, we could not detect the primary origin by fluorodeoxyglucose (FDG) positron emission tomography-computed tomography (PET-CT). Stereotactic radiotherapy was then administered, resulting in reduced tumor size and relief of symptoms. Follow-up after one year revealed an elevated CEA level (148.6 ng/mL) and remarkable fluorodeoxyglucose (FDG) uptake in the right adrenal gland, with an area of enhancement of 20 mm, on FDG-positron emission tomography computed tomography, with normal findings in other distant organs. He underwent adrenalectomy, and the adrenal tumor was diagnosed as a poorly differentiated adenocarcinoma likely of lung origin based on the histopathologic and immunohistochemistry findings of cytokeratin (CK) 7 (+), CK 20 (-), thyroid transcription factor-1 (TTF-1) (+), inhibin (-), napsin A (+), prostate-specific antigen (PSA) (-), caudal type homeobox 2 (CDX-2) (-), synaptophysin (-), and p40 (-). Metastatic tumors of unknown primary origin remain latent. Aggressive treatment of these lesions can be beneficial for symptom relief, diagnosis, and prolongation of survival.
原发灶不明的癌症(CUP)脑转移(BM)和肾上腺转移(AM)的临床管理可能具有挑战性。一名73岁男性因突发偏瘫入院。除癌胚抗原(CEA)水平升高(33.8 ng/mL)外,他的实验室检查数据均正常。对比增强磁共振成像显示右侧顶叶有一个2厘米大小的环形强化肿块,肿瘤周围有广泛的血管源性水肿。该病变被诊断为脑转移;然而,通过氟脱氧葡萄糖(FDG)正电子发射断层扫描计算机断层扫描(PET-CT)我们无法检测到原发灶。随后进行了立体定向放射治疗,肿瘤大小缩小,症状缓解。一年后的随访显示CEA水平升高(148.6 ng/mL),FDG正电子发射断层扫描计算机断层扫描显示右侧肾上腺有明显的氟脱氧葡萄糖(FDG)摄取,强化面积为20毫米,其他远处器官未见异常。他接受了肾上腺切除术,根据细胞角蛋白(CK)7(+)、CK 20(-)、甲状腺转录因子-1(TTF-1)(+)、抑制素(-)、 napsin A(+)、前列腺特异性抗原(PSA)(-)、尾型同源框2(CDX-2)(-)、突触素(-)和p40(-)的组织病理学和免疫组化结果,肾上腺肿瘤被诊断为可能起源于肺的低分化腺癌。原发灶不明的转移性肿瘤仍然隐匿。积极治疗这些病变可能有助于缓解症状、明确诊断和延长生存期。