Department of Plastic Reconstructive and Aesthetic Surgery, University of Health Sciences Gülhane Faculty of Medicine, Ankara-Türkiye.
Plastic Surgeon, Private Practice Antalya-Türkiye.
Ulus Travma Acil Cerrahi Derg. 2022 Aug;28(8):1043-1051. doi: 10.14744/tjtes.2022.68353.
Delayed autologous nerve graft reconstruction is inevitable in devastating injuries. Delayed or prolonged repair time has deleterious effects on nerve grafts. We aimed improving and accelerating nerve graft reconstruction process in a rat long nerve defect model with loop nerve graft prefabrication particularly to utilize for injuries with tissue loss.
Twenty-four Sprague-Dawley rats were allocated into three groups. 1.5 cm long peroneal nerve segment was excised, reversed in orientation, and used as autologous nerve graft. In conventional interpositional nerve graft group (Group 1), nerve defects were repaired in single-stage. In loop nerve graft prefabrication group (Group 2), grafts were sutured end-to-end (ETE) to the proximal peroneal nerve stumps. Distal ends of the grafts were sutured end-to-side to the peroneal nerve stumps 5 mm proximal to the ETE repair sites in first stage. In second stage, distal ends of the prefabricated grafts were transposed and sutured to distal nerve stumps. In staged conventional interpositional nerve graft group (Group 3), grafts were sutured ETE to proximal peroneal nerve stumps in first stage. Distal ends of the grafts and nerve stumps were tacked to the surrounding muscles until the final repair in second stage. Follow-up period was 4 weeks for each stage in Groups 2 and 3, and 8 weeks for Group 1. Peroneal function index (PFI), electrophysiology, and histological assessments were conducted after 8 weeks. P<0.05 was considered significant for statistical analysis.
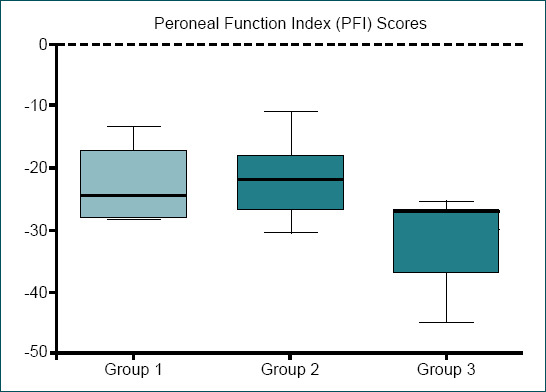
PFI results of Group 1 (-22.75±5.76) and 2 (-22.08±6) did not show statistical difference (p>0.05). Group 3 (-33.64±6.4) had a statistical difference compared to other groups (p<0.05). Electrophysiology results of Group 1 (16.19±2.15 mV/1.16±0.21 ms) and 2 (15.95±2.82 mV/1.17±0.16 ms) did not present statistical difference (p>0.05), whereas both groups had a statistical difference compared to Group 3 (10.44±1.96 mV/1.51±0.15 ms) (p<0.05). Axon counts of Group 1 (2227±260.4) and 3 (2194±201.1) did not have statistical difference (p>0.05), whereas both groups had significantly poor axon counts compared to Group 2 (2531±91.18) (p<0.05).
Loop nerve graft prefabrication improved axonal regeneration without delay. Loop prefabrication can accelerate prolonged regeneration time for the injuries indicating a delayed nerve reconstruction. Higher axon counts derived with loop nerve prefabrication may even foster its investigation in immediate long nerve defect reconstructions in further studies.
在毁灭性损伤中,延迟自体神经移植重建是不可避免的。延迟或延长修复时间对神经移植物有不良影响。我们的目的是在大鼠长神经缺损模型中改进和加速神经移植物重建过程,特别是在有组织损失的情况下使用。
将 24 只 Sprague-Dawley 大鼠分为三组。切除 1.5cm 长的腓肠神经节段,反转方向,用作自体神经移植物。在传统的间置神经移植物组(第 1 组)中,神经缺损在一期修复。在环神经移植物预制组(第 2 组)中,将移植物端对端(ETE)缝合到腓肠神经残端。在第一阶段,将移植物的远端端对侧缝合到 ETE 修复部位近端 5mm 的腓肠神经残端。在第二阶段,预制移植物的远端被移位并缝合到远端神经残端。在分期传统间置神经移植物组(第 3 组)中,第一阶段将移植物 ETE 缝合到腓肠神经残端。在第二阶段之前,将移植物的远端和神经残端缝合到周围肌肉上,直到最终修复。每组的随访时间为第 2 组和第 3 组的 4 周,第 1 组为 8 周。第 8 周后进行腓肠神经功能指数(PFI)、电生理学和组织学评估。统计分析中认为 p<0.05 具有统计学意义。
第 1 组(-22.75±5.76)和第 2 组(-22.08±6)的 PFI 结果无统计学差异(p>0.05)。第 3 组(-33.64±6.4)与其他组有统计学差异(p<0.05)。第 1 组(16.19±2.15 mV/1.16±0.21 ms)和第 2 组(15.95±2.82 mV/1.17±0.16 ms)的电生理学结果无统计学差异(p>0.05),但与第 3 组(10.44±1.96 mV/1.51±0.15 ms)有统计学差异(p<0.05)。第 1 组(2227±260.4)和第 3 组(2194±201.1)的轴突计数无统计学差异(p>0.05),但与第 2 组(2531±91.18)相比,两组的轴突计数均明显较差(p<0.05)。
环神经移植物预制可改善无延迟的轴突再生。环预制可加速延迟神经重建的延长再生时间。通过环神经预制获得的更高轴突计数甚至可能在进一步的研究中促进其在即时长神经缺损重建中的研究。