University of Cambridge, Cambridge, UK.
Cambridge University Hospitals NHS Trust, Cambridge, UK.
Clin Endocrinol (Oxf). 2022 Dec;97(6):755-762. doi: 10.1111/cen.14806. Epub 2022 Aug 17.
Familial partial lipodystrophy type 2 (FPLD2) results from autosomal dominant mutations in the LMNA gene, causing lack of subcutaneous fat deposition and excess ectopic fat accumulation, leading to metabolic complications and reduced life expectancy. The rarity of the condition means that the natural history of FPLD2 throughout childhood is not well understood. We report outcomes in a cohort of 12 (5M) children with a genetic diagnosis of FPLD2, under the care of the UK National Severe Insulin Resistance Service (NSIRS) which offers multidisciplinary input including dietetic, in addition to screening for comorbidities.
To describe the natural history of clinical, biochemical and radiological outcomes of children with FPLD2.
A retrospective case note review of children with a genetic diagnosis of FPLD2 who had been seen in the paediatric NSIRS was performed.
Twelve (5M) individuals diagnosed with FPLD2 via genetic testing before age 18 and who attended the NSIRS clinic were included.
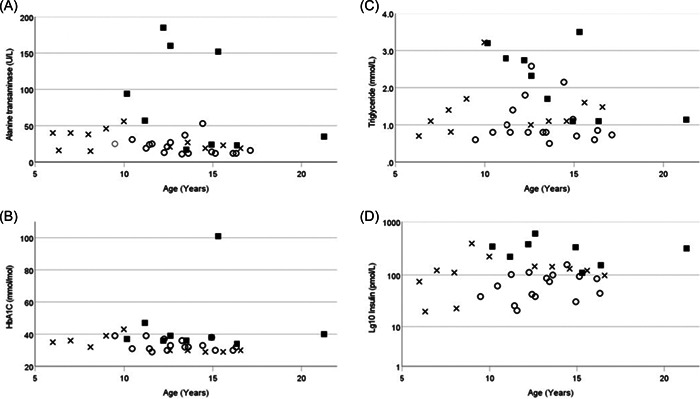
Relationships between metabolic variables (HbA1c, triglycerides, fasting insulin, fasting glucose and alanine transaminase [ALT]) across time, from first visit to most recent, were explored using a multivariate model, adjusted for age and gender. The age of development of comorbidities was recorded.
Three patients (all female) developed diabetes between 12 and 19 years and were treated with Metformin. One female has hypertrophic cardiomyopathy and four (1M) patients developed mild hepatic steatosis at a median [range] age of 14(12-15) years. Three (1M) patients reported mental health problems related to lipodystrophy. There was no relationship between biochemical results and age. Patients with diabetes had higher concentrations of ALT than patients who did not have diabetes, adjusted for age, gender and body mass index standard deviation scores.
Despite dietetic input, some patients, more commonly females, developed comorbidities after the age of 10. The absence of relationships between biochemical results and age likely reflects a small cohort size. We propose that, while clinical review and dietetic support are beneficial for children with FPLD2, formal screening for comorbidities before age 10 may not be of benefit. Clinical input from an multidisciplinary team including dietician, psychologist and clinician should be offered after diagnosis.
家族性部分脂肪营养不良 2 型(FPLD2)是由常染色体显性突变引起的,导致皮下脂肪沉积缺乏和异位脂肪过度积累,导致代谢并发症和预期寿命缩短。由于这种疾病的罕见性,儿童时期 FPLD2 的自然病史尚不清楚。我们报告了在英国国家严重胰岛素抵抗服务(NSIRS)接受治疗的 12 名(5 男)有遗传诊断为 FPLD2 的儿童队列的结果,该服务提供了包括饮食在内的多学科输入,此外还筛查了合并症。
描述 FPLD2 儿童的临床、生化和影像学结果的自然病史。
对在儿科 NSIRS 就诊的遗传诊断为 FPLD2 的儿童的病历进行回顾性病例分析。
12 名(5 男)个体通过基因检测在 18 岁之前被诊断为 FPLD2,并在 NSIRS 诊所就诊。
使用多元模型探索从第一次就诊到最近一次就诊时代谢变量(HbA1c、甘油三酯、空腹胰岛素、空腹血糖和丙氨酸氨基转移酶[ALT])之间的关系,该模型针对年龄和性别进行了调整。记录合并症发展的年龄。
3 名患者(均为女性)在 12 至 19 岁之间被诊断为糖尿病,并接受二甲双胍治疗。一名女性患有肥厚型心肌病,4 名(1 男)患者在 14(12-15)岁时被诊断为轻度肝脂肪变性。3 名(1 男)患者报告与脂肪营养不良有关的心理健康问题。生化结果与年龄之间没有关系。患有糖尿病的患者的 ALT 浓度高于没有糖尿病的患者,调整了年龄、性别和体重指数标准差分数。
尽管进行了饮食干预,但一些患者(更常见的是女性)在 10 岁后出现了合并症。生化结果与年龄之间缺乏关系可能反映了样本量较小。我们建议,虽然 FPLD2 患儿的临床检查和饮食支持是有益的,但在 10 岁之前进行合并症筛查可能没有益处。应在诊断后提供包括营养师、心理学家和临床医生在内的多学科团队的临床输入。