Colyer Jessica, Ring Lisa, Gallagher Sarah, Mullenholz Mary, Robison Jan, Rigney-Radford Kathleen, Harahsheh Ashraf S
Department of Cardiology, Seattle Children's Hospital, Seattle, WA.
Division of Cardiology, Children's National Hospital, Washington, DC.
Pediatr Qual Saf. 2022 Aug 1;7(4):e587. doi: 10.1097/pq9.0000000000000587. eCollection 2022 Jul-Aug.
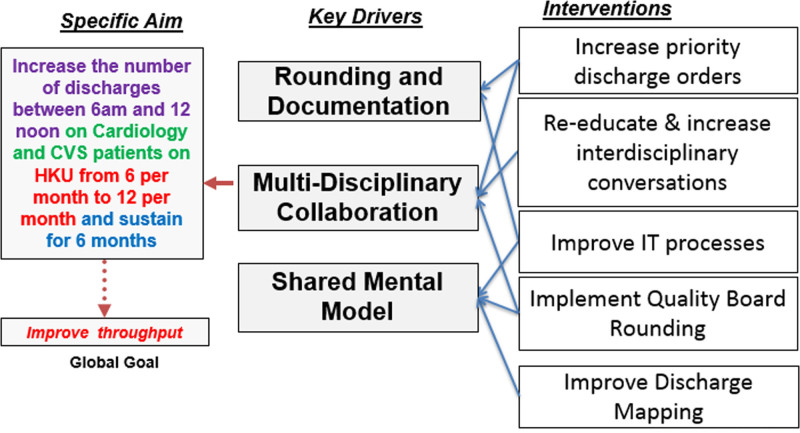
Discharging patients from the acute care setting is complex and requires orchestration of many clinical and technical processes. Focusing on timely discharges improves throughput by off-loading ICUs and coordinating safe outpatient transitions. Our data review demonstrated most discharges occurred later in the day. We sought to improve our discharge times for cardiology and cardiovascular surgery (CVS) patients in our 26-bed inpatient acute care cardiology unit (ACCU). We aimed to increase the number of discharges between 6 am and 12 pm for cardiology and CVS patients on ACCU from 5 to 10 patients per month over 6 months and sustain.
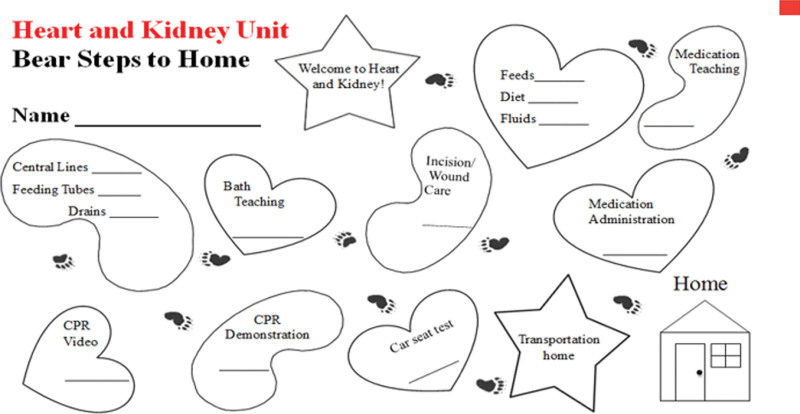
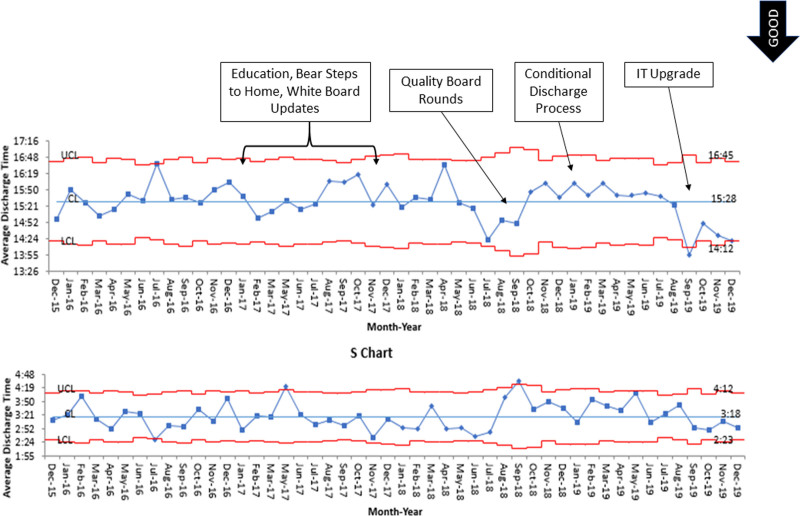
We performed a simplified Failure Mode Effect Analysis on the discharge process and identified improvement opportunities. Our key drivers centered around education, documentation, and planning. Our interventions included: staff education, communication of discharge expectations, daily quality board rounds, hospital-wide collaboration emphasizing conditional discharges, and hospital information technology (IT) improvements. We utilized statistical process control charts to analyze the data.
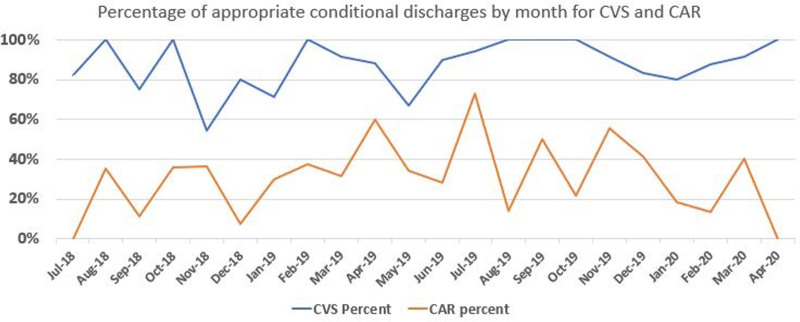
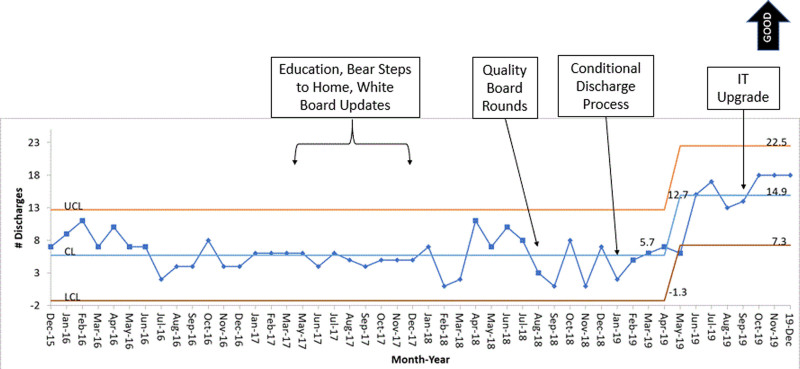
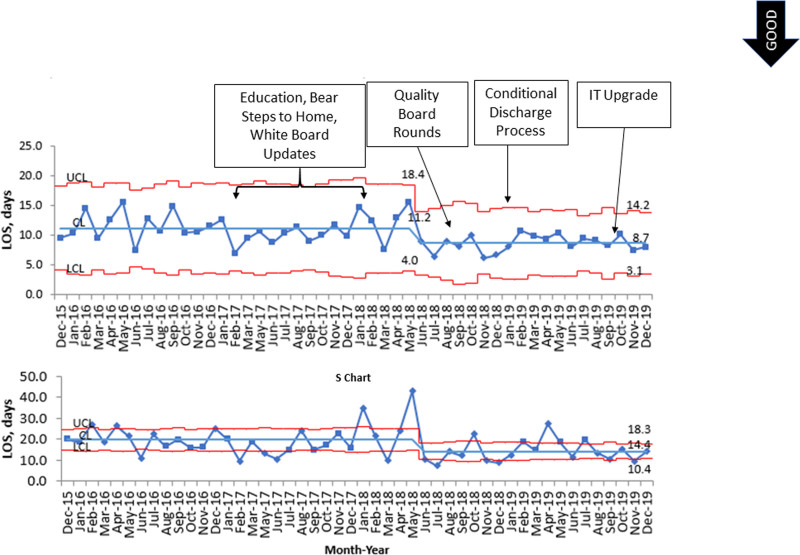
Discharges between 6 am, and 12 pm increased from a baseline of 5 (8%) to 12 (18%) patients per month with a centerline shift. Our process measures demonstrated appropriate conditional discharge usage linked to earlier discharges. Upgrades to our EMR, documentation further increased our timely discharges. Our efforts resulted in a 22% reduction in hospital length of stay from 11.2 to 8.7 days without increased readmission rates suggesting that improved efficiency did not impact care quality.
We successfully show how multidisciplinary collaboration and systems-based improvement can increase the number of safe, early discharges.
将患者从急性护理环境中出院是复杂的,需要协调许多临床和技术流程。关注及时出院可通过减轻重症监护病房负担和协调安全的门诊过渡来提高吞吐量。我们的数据审查表明,大多数出院发生在当天晚些时候。我们试图改善我们26张床位的住院急性护理心脏病单元(ACCU)中心脏病学和心血管外科(CVS)患者的出院时间。我们的目标是在6个月内将ACCU上心脏病学和CVS患者在上午6点至中午12点之间的出院人数从每月5名增加到10名,并保持这一水平。
我们对出院流程进行了简化的失效模式影响分析,并确定了改进机会。我们的关键驱动因素集中在教育、文档记录和规划方面。我们的干预措施包括:员工教育、传达出院期望、每日质量查房、全院范围内强调有条件出院的协作以及医院信息技术(IT)改进。我们使用统计过程控制图来分析数据。
上午6点至中午12点之间的出院人数从基线的每月5名(8%)增加到12名(18%),中心线发生了偏移。我们的流程措施表明,与更早出院相关的有条件出院使用得当。电子病历的升级和文档记录进一步增加了我们的及时出院人数。我们的努力使住院时间从11.2天减少了22%,降至8.7天,且再入院率没有增加,这表明效率的提高并未影响护理质量。
我们成功展示了多学科协作和基于系统的改进如何能够增加安全、早期出院的人数。