Yamazaki Hiroki, Fujinaka Toshiyuki, Ozaki Tomohiko, Kidani Tomoki, Nishimoto Keisuke, Taki Kowashi, Nishizawa Naoki, Murakami Keijiro, Kanemura Yonehiro, Nakajima Shin
Department of Neurosurgery, National Hospital Organization Osaka National Hospital, Osaka, Japan.
Surg Neurol Int. 2022 Jul 22;13:322. doi: 10.25259/SNI_529_2022. eCollection 2022.
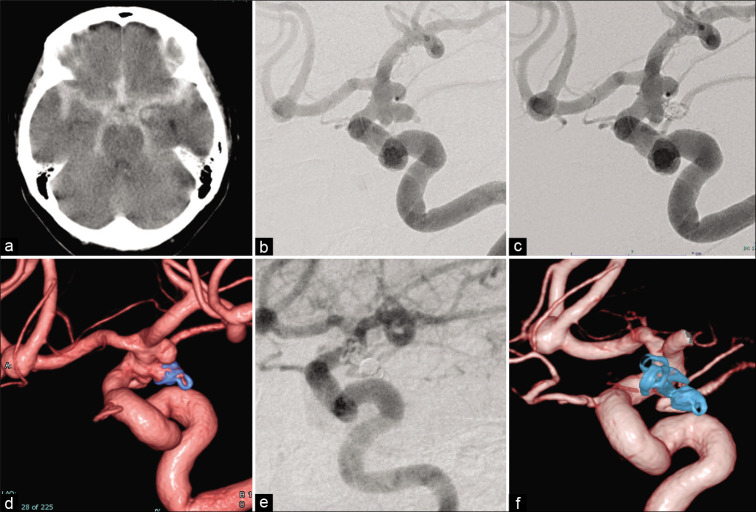
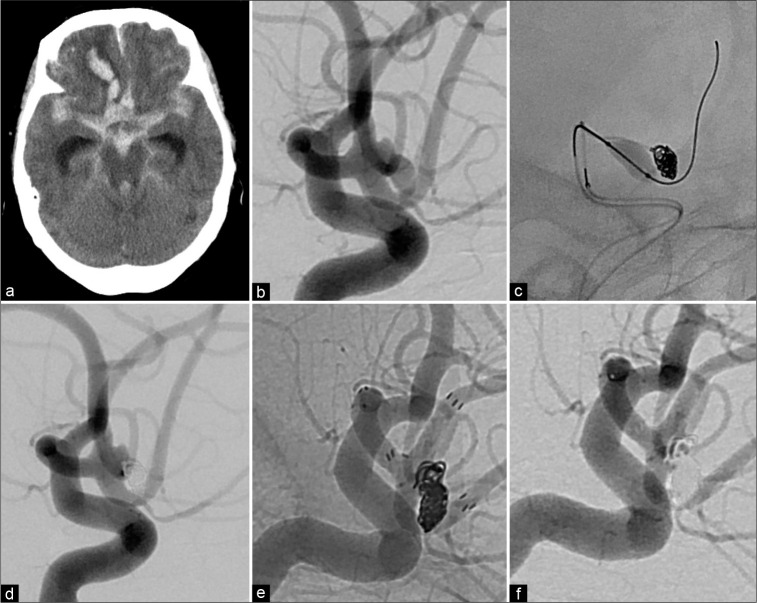
Evidence supports endovascular coiling for ruptured intracranial aneurysms (RIAs). However, in some cases, it is difficult to achieve complete occlusion by coiling, such as with wide-neck aneurysms. We report our experience with intentional staged RIA treatment using targeted endovascular coiling at the rupture point in the acute phase, followed by delayed stent-assisted coiling, flow diverter stenting, or surgical clipping.
Consecutive patients with RIAs treated between April 2015 and June 2021 were retrospectively investigated. Clinical characteristics, treatment complications, and patient outcomes data were collected.
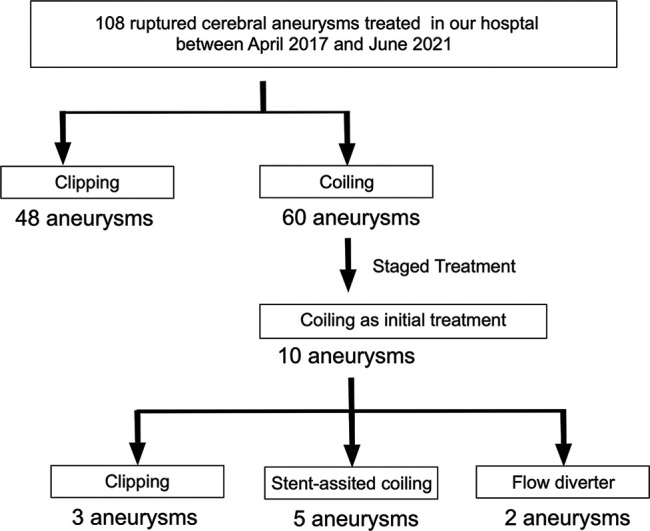
Among 108 RIAs treated in our hospital, 60 patients underwent initial coiling; 10 patients underwent staged treatment. The aneurysm locations were the anterior communicating artery ( = 5), internal carotid-posterior communicating artery ( = 3), internal carotid-paraclinoid ( = 1), and vertebral artery-posterior inferior cerebellar artery ( = 1). The mean ± standard deviation aneurysmal diameter was 9.6 ± 5.4 mm and the mean aspect ratio was 1.2 ± 0.7. As the second treatment to obliterate blood flow to the neck area, we performed five stent-assisted coiling, two flow-diverter stentings, and three surgical clippings. Only one minor perioperative complication occurred. The median duration between the first and second treatments was 18 days (range, 14- 42 days). Good clinical outcome (modified Rankin scale score 0-2) at 90 days was achieved in 5 (50%) cases. The median follow-up duration was 6.5 months (range, 3-35 months); no rerupture occurred.
Intentional staged treatment with a short time interval for RIA was effective and feasible.
有证据支持对破裂颅内动脉瘤(RIA)进行血管内栓塞治疗。然而,在某些情况下,如宽颈动脉瘤,通过栓塞难以实现完全闭塞。我们报告了我们使用急性期在破裂点进行靶向血管内栓塞,随后进行延迟支架辅助栓塞、血流导向支架置入或手术夹闭的方法对RIA进行分期治疗的经验。
回顾性研究2015年4月至2021年6月期间连续治疗的RIA患者。收集临床特征、治疗并发症和患者预后数据。
在我院治疗的108例RIA中,60例患者接受了初始栓塞;10例患者接受了分期治疗。动脉瘤位置为前交通动脉(=5)、颈内动脉-后交通动脉(=3)、颈内动脉-床突旁(=1)和椎动脉-小脑后下动脉(=1)。动脉瘤平均直径±标准差为9.6±5.4mm,平均纵横比为l.2±0.7。作为闭塞颈部区域血流的第二次治疗,我们进行了5次支架辅助栓塞、2次血流导向支架置入和3次手术夹闭。仅发生1例轻微围手术期并发症。第一次和第二次治疗之间的中位间隔时间为18天(范围14 - 42天)。90天时5例(50%)患者获得良好临床结局(改良Rankin量表评分0 - 2)。中位随访时间为6.5个月(范围3 - 35个月);未发生再破裂。
对RIA进行短时间间隔的分期治疗是有效且可行的。