Song Qi-Sheng, Zheng Cun-Jing, Wang Kun-Peng, Huang Xi-Ling, Tartakovsky Michael, Wáng Yì Xiáng J
Department of Internal Medicine, Dalian Public Health Clinical Center, Dalian, China.
Department of Imaging and Interventional Radiology, Faculty of Medicine, The Chinese University of Hong Kong, Shatin, New Territories, Hong Kong, China.
J Thorac Dis. 2022 Jul;14(7):2522-2531. doi: 10.21037/jtd-22-145.
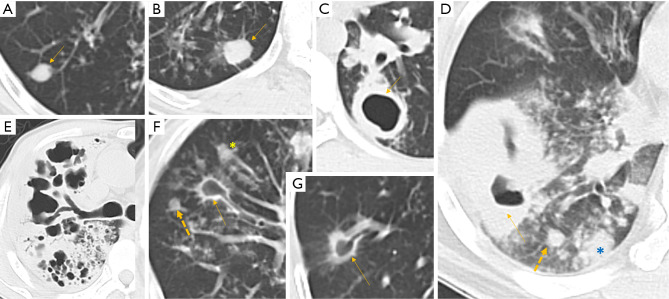
There have been concerns that literature described radiological feature differences between drug-sensitive pulmonary tuberculosis (DS-PTB) and multidrug-resistant (MDR)-PTB were confounded by that MDR-PTB cases tend to have a longer history. Using history length matched DS-PTB and MDR-PTB cases from a well-defined urban region in Dalian, we retrospectively analysed the CT feature differences of these paired cases with a focus on pulmonary nodular (PN) consolidation and pulmonary cavity (PC).
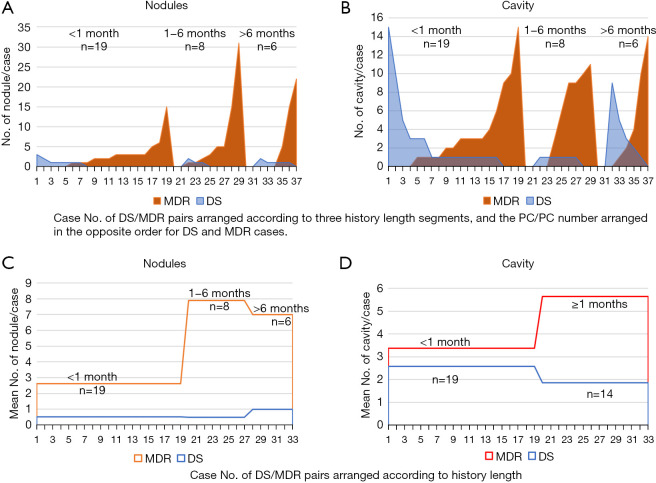
There were 33 consecutive MDR-PTB cases [inclusive of rifampicin-resistant (RR) cases, 27 males and 6 females, mean age: 49.2 years], with 19 cases had a history of <1 month and 8 and 6 cases had a history of 1-6 and >6 months respectively. To pair the MDR-PTB cases with history length, matched 33 cases of DS-PTB patients (21 males and 12 females, mean age: 56.5 years) were included. All patients were new PTB without HIV infection. The first CT exams prior to treatment were analysed.
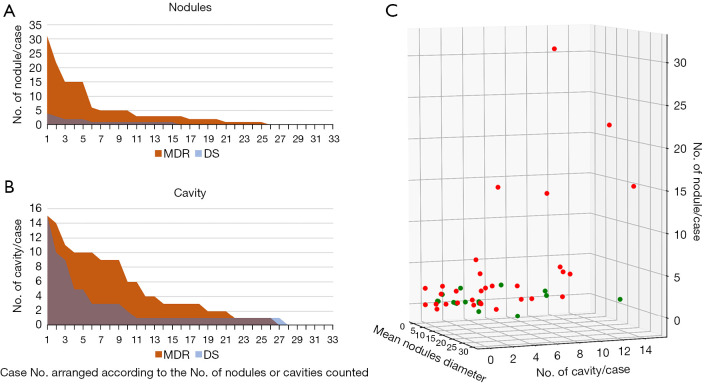
Compared with DS cases, MDR cases had a much higher prevalence of PN (75.76% 45.45%) and a higher number of PN per positive case for PN (6.2 1.53). For the cases >1 month history, MDR-PTB had a higher number of PC per positive case than that of DS-PTB cases (7.18 2.36). To differentiate DS-PTB from MDR-PTB, receiver operating characteristic (ROC) analysis showed a cutoff PN number of ≥3 had 48.5% sensitivity and 93.9% specificity, and a cutoff PC number of ≥4 had 39.4% sensitivity and 84.9% specificity. The lung field distribution of all lesions tended to be wider for MDR-PTB cases. MDR-PTB cases appeared to be associated with a faster progression in the absence of treatment.
MDR-TB is likely intrinsically more invasive than DS-TB. Multiple PN and Multiple PC are promising signs for the suspicion of MDR-PTB on chest imaging.
一直有人担心,文献中所描述的药物敏感型肺结核(DS-PTB)和耐多药肺结核(MDR-PTB)之间的放射学特征差异,因MDR-PTB病例往往病程更长而受到混淆。我们利用来自大连一个明确界定的市区、病程长度匹配的DS-PTB和MDR-PTB病例,回顾性分析了这些配对病例的CT特征差异,重点关注肺结节(PN)实变和肺空洞(PC)。
连续纳入33例MDR-PTB病例[包括耐利福平(RR)病例,男27例,女6例,平均年龄:49.2岁],其中19例病程<1个月,8例病程为1 - 6个月,6例病程>6个月。为使MDR-PTB病例与病程长度匹配,纳入了33例配对的DS-PTB患者(男21例,女12例,平均年龄:56.5岁)。所有患者均为新发肺结核且无HIV感染。分析治疗前的首次CT检查结果。
与DS病例相比,MDR病例的PN患病率更高(75.76%对45.45%),且每个PN阳性病例的PN数量更多(6.2对1.53)。对于病程>1个月的病例,MDR-PTB每个阳性病例的PC数量高于DS-PTB病例(7.18对2.36)。为鉴别DS-PTB和MDR-PTB,受试者操作特征(ROC)分析显示,PN数量截断值≥3时,敏感性为48.5%,特异性为93.9%;PC数量截断值≥4时,敏感性为39.4%,特异性为84.9%。MDR-PTB病例所有病变的肺野分布往往更广泛。MDR-PTB病例在未治疗的情况下似乎进展更快。
MDR-TB可能本质上比DS-TB更具侵袭性。多个PN和多个PC是胸部影像学上怀疑MDR-PTB的有前景的征象。