Liang Lifeng, Sun Jiayi, Chen Lizhu, Li Zejian, Zhang Wenjuan
Department of Cardiology, Tianjin Medical University General Hospital, Tianjin, China.
J Thorac Dis. 2022 Jul;14(7):2665-2676. doi: 10.21037/jtd-22-833.
Congestive heart failure (HF) is a common condition in the intensive care unit (ICU). Cardiomyopathy is an important etiological factor in HF. However, few studies have explored the effect of cardiomyopathy on the prognosis of HF. This study explored the association between comorbid cardiomyopathy and the outcomes of critically ill patients with congestive HF.
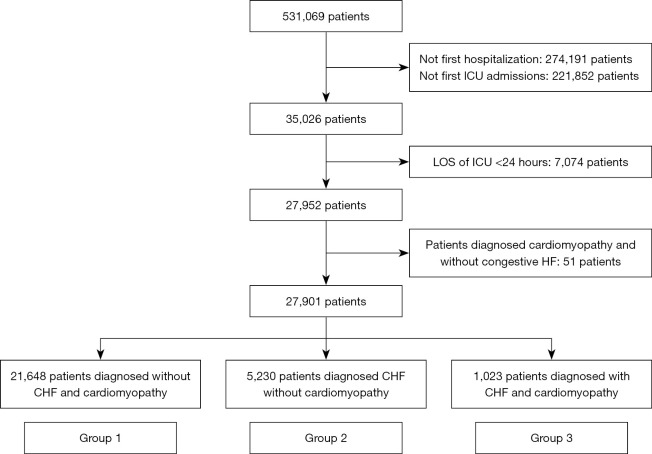
A retrospective cohort study was performed using data extracted from Medical Information Mart for Intensive Care IV (MIMIC-IV) database. All adult patients with the first ICU admission were enrolled as participants but those diagnosed with cardiomyopathy alone were excluded. The demographics, comorbidities, vital signs, laboratory tests, scoring systems, and treatments of patients were extracted to further analyze. The composite endpoints included in-hospital mortality, cardiac arrest, and re-admission to the ICU. The association between cardiomyopathy comorbidity and the composite endpoints was assessed using propensity-score matching (PSM) and multivariable logistic regression models.
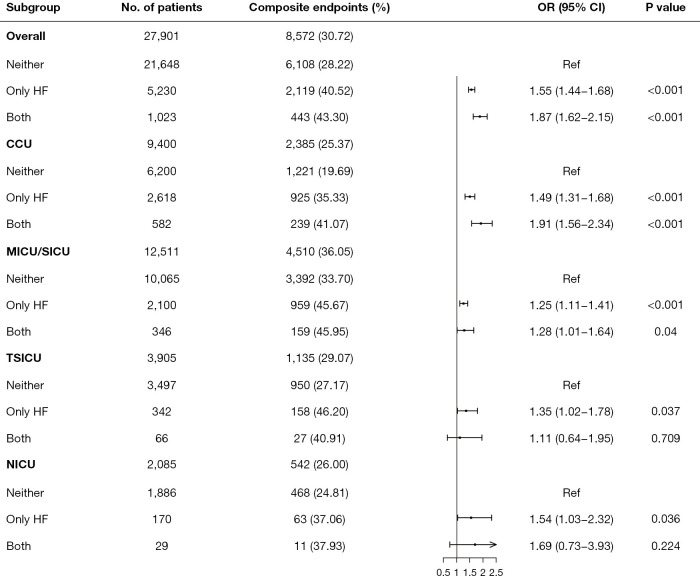
A total of 27,901 critically ill patients were enrolled, including 1,023 patients diagnosed with cardiomyopathy and congestive HF. The average age of the cohort was 64.37±17.36 years, and 58.13% of the patients were men. The ethnicity of patients was mainly white (64.67%). Multivariable logistic regression analyses found the risk of composite endpoints in patients with cardiomyopathy was higher than other groups [odds ratio (OR) =1.87; 95% confidence interval (CI): 1.62-2.15; P<0.001]. Compared to patients with congestive HF alone (OR =1.43; 95% CI: 1.26-1.62; P<0.001), patients with cardiomyopathy had a similar risk of in-hospital death (OR =1.35; 95% CI: 1.06-1.71; P=0.014). Moreover, the risks of cardiac arrest (OR =1.53; 95% CI: 1.01-2.34; P=0.029) and re-admission to the ICU (OR =1.74; 95% CI: 1.39-2.17; P<0.001) were both higher in patients with cardiomyopathy than other groups. After PSM, the risk of composite endpoints was still higher in patients with cardiomyopathy (OR =1.64; 95% CI: 1.33-2.02; P<0.001). The association was consistent among patients admitted to the coronary care unit (CCU) and medical ICU (MICU)/surgical ICU (SICU).
Comorbid cardiomyopathy increased the risk of composite endpoints in patients with congestive HF admitted to the ICU. Cardiomyopathy is related to the poor outcomes of critically ill patients with congestive HF.
充血性心力衰竭(HF)是重症监护病房(ICU)中的常见病症。心肌病是HF的一个重要病因。然而,很少有研究探讨心肌病对HF预后的影响。本研究探讨了合并心肌病与重症充血性HF患者结局之间的关联。
进行一项回顾性队列研究,使用从重症监护医学信息数据库IV(MIMIC-IV)中提取的数据。所有首次入住ICU的成年患者均纳入研究,但单独诊断为心肌病的患者除外。提取患者的人口统计学、合并症、生命体征、实验室检查、评分系统和治疗方法以进行进一步分析。复合终点包括院内死亡率、心脏骤停和再次入住ICU。使用倾向评分匹配(PSM)和多变量逻辑回归模型评估合并心肌病与复合终点之间的关联。
共纳入27901例重症患者,其中1023例诊断为心肌病合并充血性HF。队列的平均年龄为64.37±17.36岁,58.13%的患者为男性。患者的种族主要为白人(64.67%)。多变量逻辑回归分析发现,心肌病患者发生复合终点的风险高于其他组[比值比(OR)=1.87;95%置信区间(CI):1.62 - 2.15;P<0.001]。与单纯充血性HF患者相比(OR =1.43;95%CI:1.26 - 1.62;P<0.001),心肌病患者的院内死亡风险相似(OR =1.35;95%CI:1.06 - 1.71;P=0.014)。此外,心肌病患者的心脏骤停风险(OR =1.53;95%CI:1.01 - 2.34;P=0.029)和再次入住ICU的风险(OR =1.74;95%CI:1.39 - 2.17;P<0.001)均高于其他组。PSM后,心肌病患者发生复合终点的风险仍然较高(OR =1.64;95%CI:1.33 - 2.02;P<0.001)。在冠心病监护病房(CCU)和内科ICU(MICU)/外科ICU(SICU)收治的患者中,这种关联是一致的。
合并心肌病增加了入住ICU的充血性HF患者发生复合终点的风险。心肌病与重症充血性HF患者不良结局相关。