Department of Urology, Nippon Medical School Hospital, 1-1-5, Sendagi, Bunkyo-ku, Tokyo, 113-8603, Japan.
Department of Radiology, Nippon Medical School Hospital, 1-1-5, Sendagi, Bunkyo-ku, Tokyo, 113-8603, Japan.
BMC Cancer. 2022 Aug 5;22(1):856. doi: 10.1186/s12885-022-09971-w.
Active surveillance (AS) is one of the treatment methods for patients with small renal masses (SRMs; < 4 cm), including renal cell carcinomas (RCCs). However, some small RCCs may exhibit aggressive neoplastic behaviors and metastasize. Little is known about imaging biomarkers capable of identifying potentially aggressive small RCCs. Contrast-enhanced computed tomography (CECT) often detects collateral vessels arising from neoplastic angiogenesis in RCCs. Therefore, this study aimed to evaluate the association between SRM differential diagnoses and prognoses, and the detection of collateral vessels using CECT.
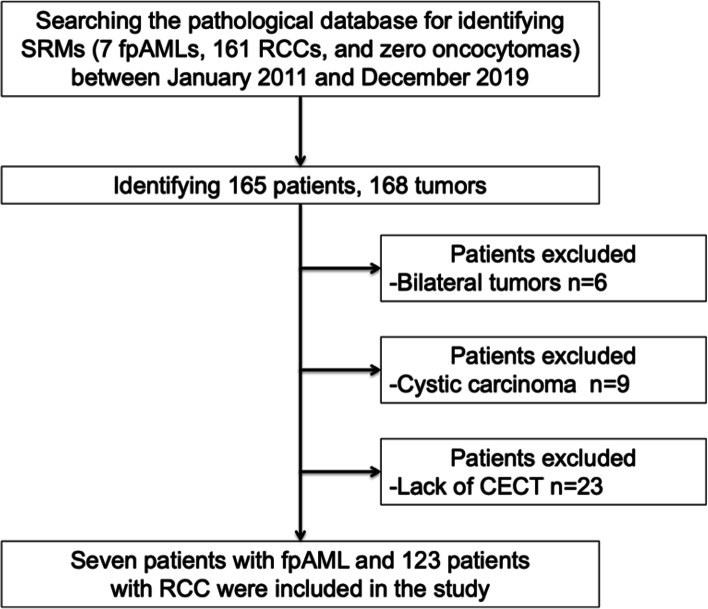
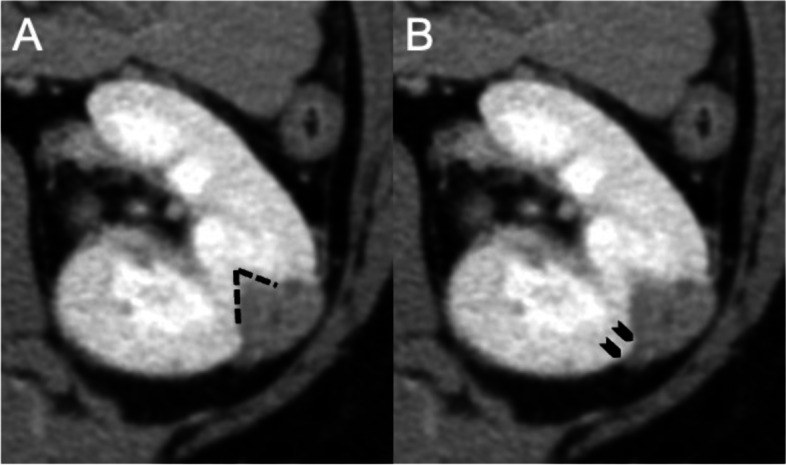
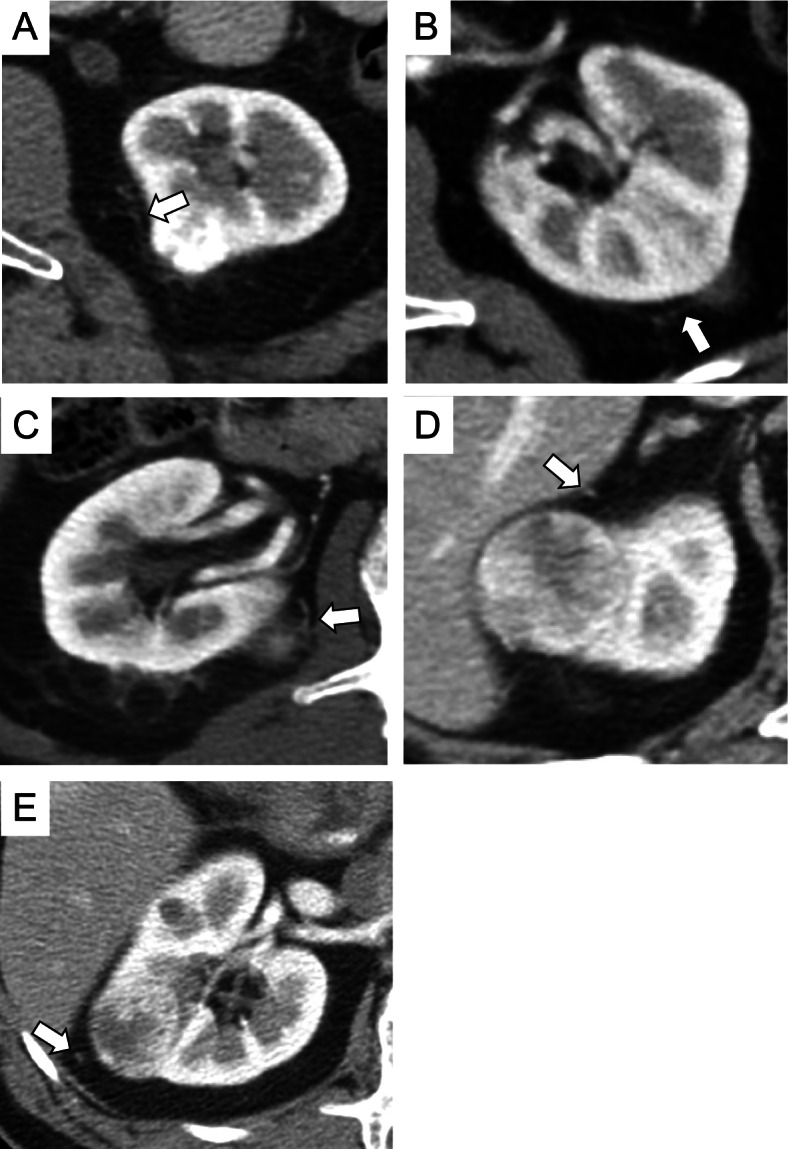
A total of 130 consecutive patients with pathologically confirmed non-metastatic SRMs (fat-poor angiomyolipomas [fpAMLs; n = 7] and RCCs [n = 123]) were retrospectively enrolled. Between 2011 and 2019, SRM diagnoses in these patients were confirmed after biopsy or surgical resection. All RCCs were surgically resected. Regardless of diameter, a collateral vessel (CV) was defined as any blood vessel connecting the tumor from around the kidney using CECT. First, we analyzed the role of CV-detection in differentiating between fpAML and RCC. Then, we evaluated the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of RCC diagnosis based on CV-detection using CECT. We also assessed the prognostic value of CV-detection using the Fisher exact test, and Kaplan-Meier method and the log-rank test.
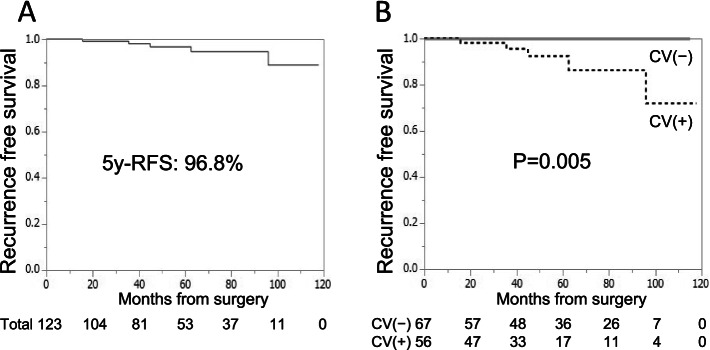
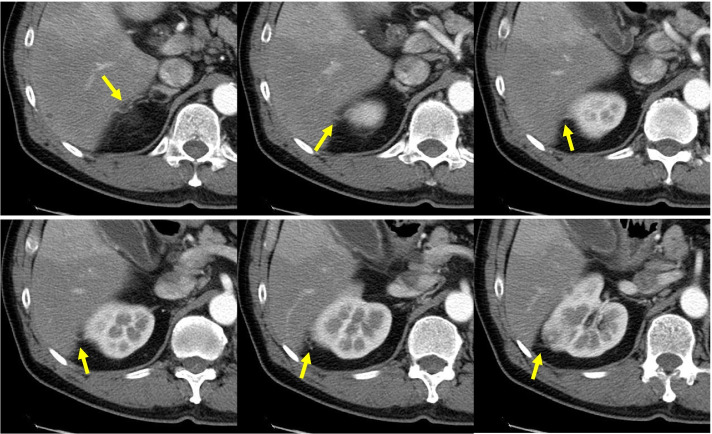
The sensitivity, specificity, PPV, NPV, and accuracy of CV-detection for the diagnosis of small RCCs was 48.5, 45.5, 100, 100, and 9.5% respectively. Five of 123 (4.1%) patients with RCC experienced recurrence. CV-detection using CECT was the only significant factor associated with recurrence (p = 0.0177). Recurrence-free survival (RFS) was significantly lower in patients with CV compared with in those without CV (5-year RFS 92.4% versus 100%, respectively; p = 0.005). In addition, critical review of the CT images revealed the CVs to be continuous with the venous vessels around the kidney.
The detection of CVs using CECT is useful for differentiating between small fpAMLs and RCCs. CV-detection may also be applied as a predictive parameter for small RCCs prone to recurrence after surgical resection. Moreover, AS could be suitable for small RCCs without CVs.
主动监测(AS)是治疗小肾肿块(SRM;<4cm)患者的方法之一,包括肾细胞癌(RCC)。然而,一些小的 RCC 可能表现出侵袭性的肿瘤行为并转移。目前尚不清楚哪些影像学生物标志物能够识别出具有潜在侵袭性的小 RCC。增强 CT(CECT)常用于检测 RCC 中新生血管的侧支血管。因此,本研究旨在评估 SRM 鉴别诊断与预后以及 CECT 检测侧支血管之间的相关性。
回顾性纳入 2011 年至 2019 年间经病理证实的非转移性 SRM(乏脂性血管平滑肌脂肪瘤[fpAMLs;n=7]和 RCC[n=123])的 130 例连续患者。在这些患者中,SRM 的诊断通过活检或手术切除得到确认。所有 RCC 均经手术切除。使用 CECT,直径不限,将任何连接肾脏周围肿瘤的血管定义为侧支血管(CV)。首先,我们分析了 CECT 检测 CV 在鉴别 fpAML 和 RCC 中的作用。然后,我们评估了基于 CECT 检测 CV 对 RCC 诊断的敏感性、特异性、阳性预测值(PPV)、阴性预测值(NPV)和准确性。我们还使用 Fisher 精确检验、Kaplan-Meier 方法和对数秩检验评估了 CV 检测的预后价值。
CECT 检测 CV 对小 RCC 诊断的敏感性、特异性、PPV、NPV 和准确性分别为 48.5%、45.5%、100%、100%和 9.5%。123 例 RCC 患者中有 5 例(4.1%)复发。CECT 检测 CV 是唯一与复发相关的显著因素(p=0.0177)。有 CV 的患者无复发生存率(RFS)明显低于无 CV 的患者(5 年 RFS 分别为 92.4%和 100%;p=0.005)。此外,对 CT 图像的仔细审查显示 CV 与肾脏周围的静脉血管连续。
CECT 检测 CV 有助于鉴别小的 fpAML 和 RCC。CV 检测也可用作预测小 RCC 术后易复发的参数。此外,对于没有 CV 的小 RCC,AS 可能是合适的。