Wachinger Jonas, McMahon Shannon A, Lohmann Julia, De Allegri Manuela, Denkinger Claudia M
Heidelberg Institute of Global Health, Heidelberg University Hospital, 69120 Heidelberg, Germany.
Division of Clinical Tropical Medicine, Center of Infectious Diseases, Heidelberg University Hospital, 69120 Heidelberg, Germany.
SSM Qual Res Health. 2022 Dec;2:100140. doi: 10.1016/j.ssmqr.2022.100140. Epub 2022 Jul 30.
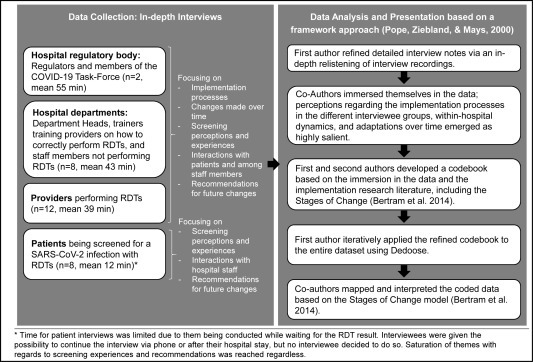
Antigen-based rapid diagnostic tests (RDTs) for SARS-CoV-2 have good reliability and have been repeatedly implemented as part of pandemic response policies, especially for screening in high-risk settings (e.g., hospitals and care homes) where fast recognition of an infection is essential. However, evidence from actual implementation efforts and associated experiences is lacking. We conducted a qualitative study at a large tertiary care hospital in Germany to identify step-by-step processes when implementing RDTs for the screening of incoming patients, as well as stakeholders' implementation experiences. We relied on 30 in-depth interviews with hospital staff (members of the regulatory body, department heads, staff working on the wards, staff training providers on how to perform RDTs, and providers performing RDTs as part of the screening) and patients being screened with RDTs. Despite some initial reservations, RDTs were rapidly accepted and adopted as the best available tool for accessible and reliable screening. Decentralized implementation efforts resulted in different procedures being operationalized across departments. Procedures were continuously refined based on initial experiences (e.g., infrastructural or scheduling constraints), pandemic dynamics (growing infection rates), and changing regulations (e.g., screening of all external personnel). To reduce interdepartmental tension, stakeholders recommended high-level, consistently communicated and enforced regulations. Despite challenges, RDT-based screening for all incoming patients was observed to be feasible and acceptable among implementers and patients, and merits continued consideration in the context of high infection and stagnating vaccination rates.
用于严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的基于抗原的快速诊断测试(RDT)具有良好的可靠性,并已作为大流行应对政策的一部分被反复采用,特别是在高风险环境(如医院和疗养院)的筛查中,快速识别感染至关重要。然而,缺乏实际实施工作和相关经验的证据。我们在德国一家大型三级护理医院进行了一项定性研究,以确定在对入院患者进行筛查时实施RDT的逐步流程,以及利益相关者的实施经验。我们对医院工作人员(监管机构成员、科室主任、病房工作人员、RDT操作培训人员以及作为筛查一部分进行RDT操作的人员)和接受RDT筛查的患者进行了30次深入访谈。尽管最初存在一些保留意见,但RDT迅速被接受并作为可及且可靠筛查的最佳可用工具采用。分散的实施工作导致各部门采用了不同的操作程序。程序根据初始经验(如基础设施或日程安排限制)、大流行动态(不断上升的感染率)和不断变化的法规(如对所有外部人员的筛查)持续完善。为了减少部门间的紧张关系,利益相关者建议制定高层级、持续沟通并严格执行的法规。尽管存在挑战,但基于RDT对所有入院患者进行筛查在实施者和患者中被认为是可行且可接受的,并且在高感染率和疫苗接种率停滞不前的情况下值得继续考虑。