Department of Internal Medicine II, University Hospital Regensburg, Regensburg, Bavaria, Germany.
Center for Clinical Studies, University Medical Center Regensburg, Regensburg, Bavaria, Germany.
PLoS One. 2022 Aug 8;17(8):e0272577. doi: 10.1371/journal.pone.0272577. eCollection 2022.
Unfractionated heparin (UFH) is the commonly used anticoagulant to prevent clotting of the ECMO circuit and thrombosis of the cannulated vessels. A side effect of UFH is heparin-induced thrombocytopenia (HIT). Little is known about HIT during ECMO and the impact of changing anticoagulation in ECMO patients with newly diagnosed HIT. The aim of the study was to determine the prevalence, complications, impact of switching anticoagulation to argatroban and outcomes of patients developing heparin-induced thrombocytopenia (HIT) during either veno-venous (VV) or veno-arterial (VA) ECMO.
Retrospective observational single centre study of prospectively collected data of consecutive patients receiving VV ECMO therapy for severe respiratory failure and VA ECMO for circulatory failure from January 2006 to December 2016 of the Medical intensive care unit (ICU) of the University Hospital of Regensburg. Treatment of HIT on ECMO was done with argatroban.
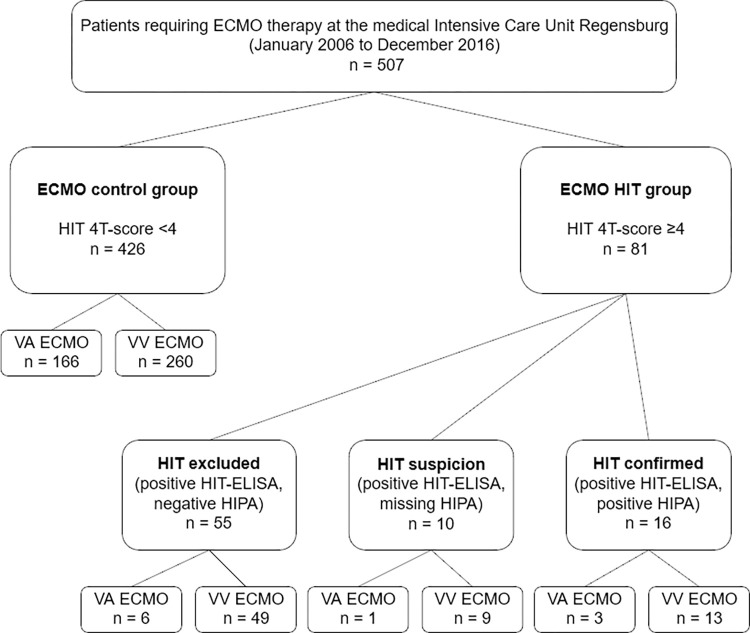
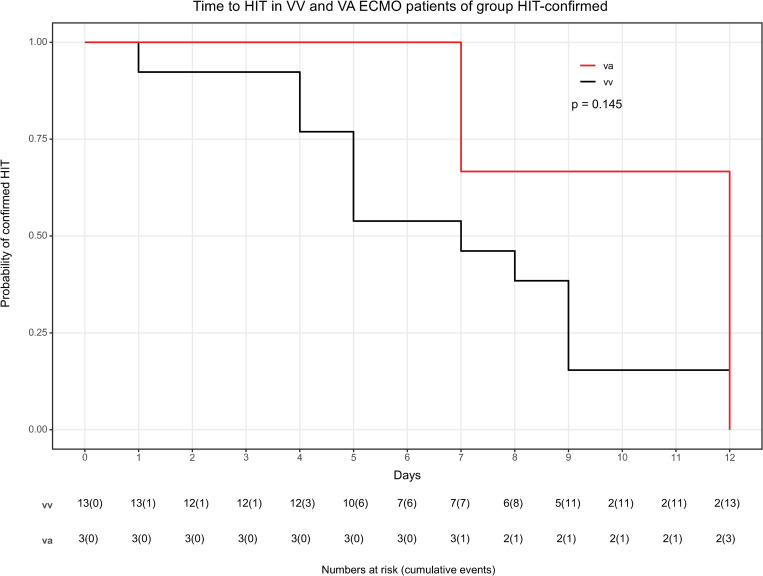
507 patients requiring ECMO were included. Further HIT-diagnostic was conducted if HIT-4T-score was ≥4. The HIT-confirmed group had positive HIT-enzyme-linked-immunosorbent-assay (ELISA) and positive heparin-induced-platelet-activation (HIPA) test, the HIT-suspicion group a positive HIT-ELISA and missing HIPA but remained on alternative anticoagulation until discharge and the HIT-excluded group a negative or positive HIT-ELISA, however negative HIPA. These were compared to group ECMO-control without any HIT suspicion. The prevalence of HIT-confirmed was 3.2%, of HIT-suspicion 2.0% and HIT-excluded 10.8%. Confirmed HIT was trendwise more frequent in VV than in VA (3.9 vs. 1.7% p = 0.173). Compared to the ECMO control group, patients with confirmed HIT were longer on ECMO (median 13 vs. 8 days, p = 0.002). Different types of complications were higher in the HIT-confirmed than in the ECMO-control group, but in-hospital mortality was not different (31% vs. 41%, p = 0.804).
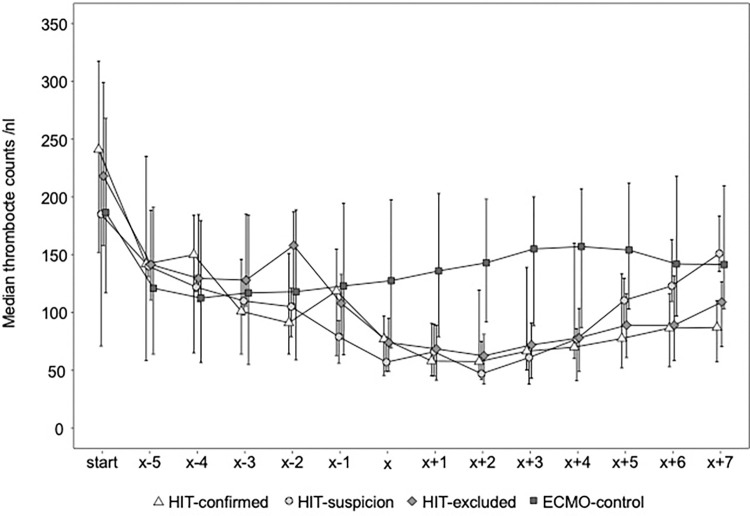
HIT is rare on ECMO, should be suspected, if platelets are decreasing, but seems not to increase mortality if treated promptly.
未分级肝素(UFH)是常用的抗凝剂,用于防止 ECMO 回路凝血和插管血管血栓形成。UFH 的副作用是肝素诱导的血小板减少症(HIT)。关于 ECMO 期间的 HIT 以及在新诊断出 HIT 的 ECMO 患者中改变抗凝治疗的影响知之甚少。本研究的目的是确定在接受静脉-静脉(VV)或静脉-动脉(VA)ECMO 治疗的严重呼吸衰竭患者中,肝素诱导的血小板减少症(HIT)的患病率、并发症、转换为阿加曲班抗凝的影响以及接受 ECMO 治疗的患者的结果。
对 2006 年 1 月至 2016 年 12 月期间在雷根斯堡大学医院重症监护病房(ICU)接受 VV ECMO 治疗严重呼吸衰竭和 VA ECMO 治疗循环衰竭的连续患者前瞻性收集的数据进行回顾性观察性单中心研究。HIT 在 ECMO 上的治疗是用阿加曲班进行的。
507 名需要 ECMO 的患者被纳入研究。如果 HIT-4T 评分≥4,则进一步进行 HIT 诊断。HIT 确诊组的 HIT-酶联免疫吸附试验(ELISA)阳性和肝素诱导的血小板活化(HIPA)试验阳性,HIT 疑似组的 HIT-ELISA 阳性且 HIPA 缺失,但在出院前仍接受替代抗凝治疗,HIT 排除组的 HIT-ELISA 阴性或阳性,但 HIPA 阴性。这些与任何 HIT 怀疑均无的 ECMO 对照组进行比较。HIT 确诊组的患病率为 3.2%,HIT 疑似组为 2.0%,HIT 排除组为 10.8%。与 VA 相比,VV 中确诊的 HIT 趋势更为频繁(3.9%比 1.7%,p=0.173)。与 ECMO 对照组相比,确诊的 HIT 患者在 ECMO 上的时间更长(中位数 13 天 vs. 8 天,p=0.002)。在 HIT 确诊组中,不同类型的并发症发生率高于 ECMO 对照组,但住院死亡率无差异(31%比 41%,p=0.804)。
HIT 在 ECMO 上很少见,如果血小板减少,应怀疑 HIT,但如果及时治疗,似乎不会增加死亡率。