Kazantsev Anton N, Zharova Alina S, Sokolova Ekaterina V, Korotkikh Alexander V
Kostroma regional clinical hospital named after E.I. Korolev, Kostroma, Russian Federation.
North-Western State Medical University. I.I. Mechnikov, St. Petersburg, Russian Federation.
Radiol Case Rep. 2022 Aug 1;17(10):3699-3708. doi: 10.1016/j.radcr.2022.07.034. eCollection 2022 Oct.
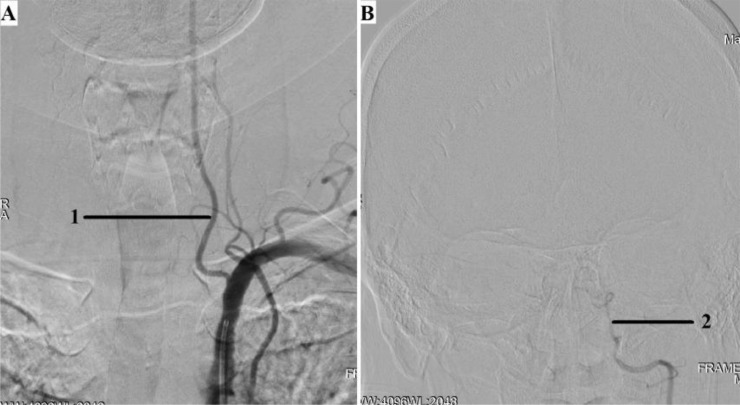
The A.N. Kazantsev artery is a vessel starting from the common carotid artery with subsequent bifurcation into 2 vessels of equal size-the internal carotid artery (ICA) and the persistent embryonic hypoglossal artery (PEHA). Until now, this artery has been considered as the ICA. However, according to all existing classifications, the ICA in the cervical segment does not have arterial branches. In addition, in view of the comparable sizes of PEHA and ICA, PEHA itself cannot be considered a branch of the ICA. Thus, by the right of the first description, the authors of the article named this vascular formation as the A.N. Kazantsev artery, which forms a bifurcation of the PEHA and ICA. In this clinical case, carotid angioplasty (CAS) was performed with stenting of 80% stenosis of the A.N. Kazantsev artery in the most acute period of acute cerebrovascular accident (ACV). According to angiography, the following was also revealed: the presence of PEHA, extending from the A.N. Kazantsev artery 5 cm above its mouth, connecting with the main artery; stenosis of the right vertebral artery 60% at the mouth; hypoplastic left vertebral artery with aplasia of the V4 segment; open circle of Willis (VC): absence of both posterior communicating arteries (PCA). Due to the high risk of recurrent CVA due to clamping of the A.N. Kazantsev artery during CEA, a multidisciplinary consultation decided to implement an emergency CAS of the A.N. Kazantsev artery. The distal embolism protection system FilterWire was inserted into the proximal part of the basilar artery through the radial artery on the left. The distal embolism protection system RX Accunet was inserted into the distal parts of the left ICA through the left common femoral artery. According to Seldinger, an Acculink stent 7-10 × 30 mm was inserted into the affected area of the A.N. Kazantsev artery, positioned and opened. The postoperative period was uneventful. ACV did not recur. Conducted dual antiplatelet therapy (acetylsalicylic acid 125 mg in the afternoon + clopidogrel 75 mg in the morning). The patient was discharged from the institution on the 10th day after the operation in a satisfactory condition.
A.N. 卡赞采夫动脉是一条起始于颈总动脉的血管,随后分为两条大小相等的血管——颈内动脉(ICA)和持续存在的胚胎舌下动脉(PEHA)。到目前为止,这条动脉一直被认为是颈内动脉。然而,根据所有现有的分类,颈段的颈内动脉没有动脉分支。此外,鉴于PEHA和ICA大小相当,PEHA本身不能被视为颈内动脉的分支。因此,基于首次描述的权利,本文作者将这种血管结构命名为A.N. 卡赞采夫动脉,它形成了PEHA和ICA的分叉。在这个临床病例中,在急性脑血管意外(ACV)的最急性期,对A.N. 卡赞采夫动脉80%狭窄处进行了颈动脉血管成形术(CAS)并置入支架。根据血管造影,还发现了以下情况:PEHA存在,从A.N. 卡赞采夫动脉开口上方5厘米处发出,与主动脉相连;右椎动脉开口处狭窄60%;左椎动脉发育不全,V4段缺如;Willis环(VC)开放:双侧后交通动脉(PCA)缺如。由于在颈动脉内膜切除术(CEA)期间夹闭A.N. 卡赞采夫动脉会导致复发性CVA的高风险,多学科会诊决定对A.N. 卡赞采夫动脉实施紧急CAS。通过左侧桡动脉将远端栓塞保护系统FilterWire插入基底动脉近端。通过左侧股总动脉将远端栓塞保护系统RX Accunet插入左侧颈内动脉远端。根据Seldinger技术,将一个7 - 10×30毫米的Acculink支架插入A.N. 卡赞采夫动脉的病变部位,定位并打开。术后过程顺利。ACV未复发。进行了双联抗血小板治疗(下午服用阿司匹林125毫克 + 早上服用氯吡格雷75毫克)。患者术后第10天情况良好,从机构出院。