Department of Urology, National Center for Children's Health, Beijing Children's Hospital Affiliated to Capital Medical University, Beijing, 100045, China.
BMC Urol. 2022 Aug 10;22(1):124. doi: 10.1186/s12894-022-01080-x.
At present, there is no specific research on the factors affecting the success rate of urethroplasty in patients with DSD. The purpose of this study is to explore the factors affecting the success of urethroplasty in DSD patients, and to provide some reference for the surgical treatment of DSD patients undergoing urethroplasty.
We reviewed patients with DSD who underwent urethroplasty from January 2016 to December 2019 retrospectively. Patients were divided into four groups: the successful group, the urethrocutaneous fistula group, the urethral diverticulum group, and the urethral stricture group. Risk factors were determined from the following data included the DSD classification, the age of first operation, length of urethral defect, degree of hypospadias, cryptorchidism, micropenis, gonad type, hormone therapy before operation, transposition of penis and scrotum, surgical strategy, urethral covering material, and postoperative catheter removal time. We explored the difference of each factor between four groups through the comparative study of single factor and multifactor logistic regression analysis of related factors.
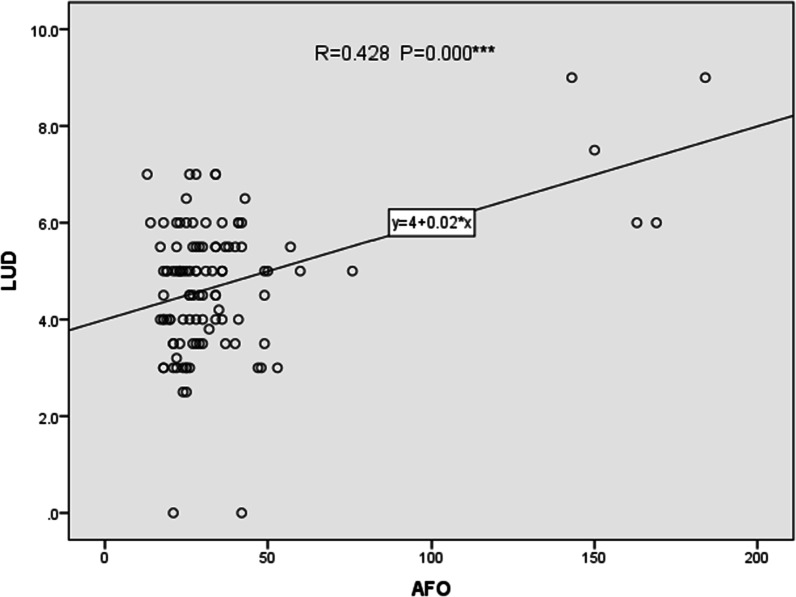
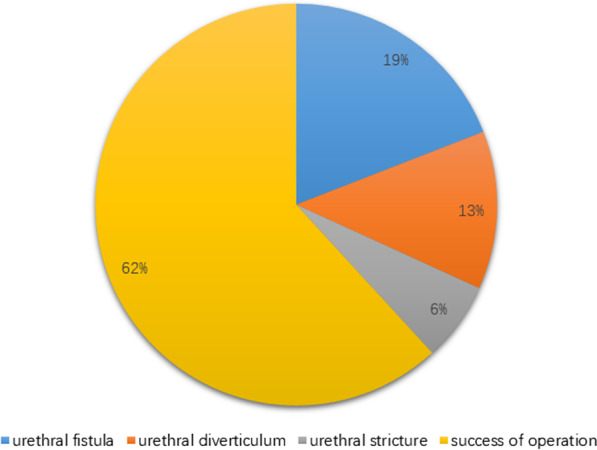
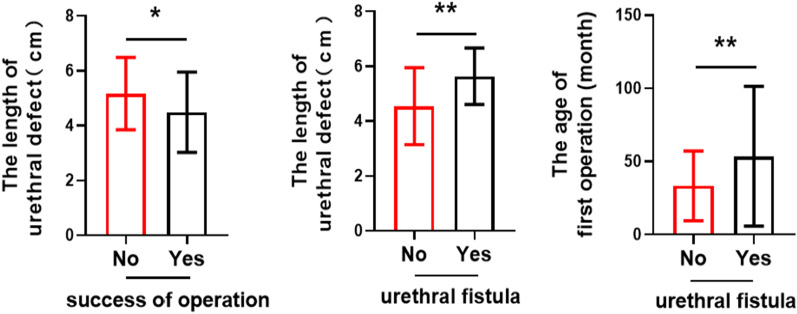
122 cases were enrolled in this group (n = 122), 12 cases were lost to follow-up. Median follow-up was 28 months (12-55 months).We found the success rate of operation decreased with longer urethral defect (B = - 0.473, P = 0.005). The success rate of operation was higher in staged operation and TPIT (TPIT = Transverse Preputial Island Tube operation)-related operation than primary operation (B = 1.238, P = 0.006) and TPIT-nonrelated operation (B = 2.293, P = 0.001). Although there was a significant difference between the age of the first operation and the occurrence of urethrocutaneous fistula (P = 0.006 < 0.05), there was no significant difference in logistic regression analysis (P = 0.161 > 0.05). The incidence of urethrocutaneous fistula was lower in TPIT-related operation than in TPIT-nonrelated operation (B = - 2.507, P = 0.000). The incidence of postoperative urethral diverticulum was lower in staged operation than in primary operation (B = - 1.737, P = 0.015).
For patients with disorder of sex development undergoing urethroplasty, the length of urethral defect is an independent risk factor affecting both the success rate of operation and the urethrocutaneous fistula. The age of the first operation has a statistically significant effect on the occurrence of postoperative urethrocutaneous fistula, but it is not an independent factor. Urethrocutaneous fistula is less found in TPIT-related operation in the study. Staged operation is an independent protective factor for postoperative urethral diverticulum compared with one-stage operation but isn't related to urethrocutaneous fistula.
目前,对于 DSD 患者尿道成形术成功率的影响因素尚无专门研究。本研究旨在探讨影响 DSD 患者尿道成形术成功率的因素,为 DSD 患者行尿道成形术的手术治疗提供参考。
回顾性分析 2016 年 1 月至 2019 年 12 月行尿道成形术的 DSD 患者。将患者分为四组:成功组、尿道皮肤瘘组、尿道憩室组和尿道狭窄组。从 DSD 分类、首次手术年龄、尿道缺损长度、尿道下裂程度、隐睾、小阴茎、性腺类型、术前激素治疗、阴茎和阴囊转位、手术策略、尿道覆盖材料和术后导尿管拔除时间等数据中确定危险因素。通过单因素比较研究和相关因素多因素逻辑回归分析,探讨了四组之间各因素的差异。
本研究共纳入 122 例患者(n=122),12 例失访。中位随访时间为 28 个月(12-55 个月)。我们发现尿道缺损越长,手术成功率越低(B=-0.473,P=0.005)。分期手术和 TPIT(横向包皮岛状管术)相关手术的手术成功率高于一期手术(B=1.238,P=0.006)和 TPIT 不相关手术(B=2.293,P=0.001)。虽然首次手术年龄与尿道皮肤瘘的发生有显著差异(P=0.006<0.05),但逻辑回归分析无显著差异(P=0.161>0.05)。TPIT 相关手术中尿道皮肤瘘的发生率低于 TPIT 不相关手术(B=-2.507,P=0.000)。分期手术中术后尿道憩室的发生率低于一期手术(B=-1.737,P=0.015)。
对于行尿道成形术的 DSD 患者,尿道缺损长度是影响手术成功率和尿道皮肤瘘的独立危险因素。首次手术年龄对术后尿道皮肤瘘的发生有统计学意义,但不是独立因素。本研究中,TPIT 相关手术中尿道皮肤瘘的发生率较低。与一期手术相比,分期手术是术后尿道憩室的独立保护因素,但与尿道皮肤瘘无关。