Department of Cardiovascular Surgery, Union Hospital, Fujian Medical University, Fujian, China; Key Laboratory of Cardio-Thoracic Surgery Fujian Medical University, Fujian Province University, Fujian, China.
Anatol J Cardiol. 2022 Nov;26(11):802-809. doi: 10.5152/AnatolJCardiol.2022.1665.
Previous studies have shown that transcatheter aortic valve implantation is the best alternative therapy to surgical aortic valve replacement in high-risk surgical patients with aortic stenosis. However, it is not clear whether transcatheter aortic valve implantation can be utilized in low-risk surgical patients with aortic stenosis. This studyaimed to evaluate the safety and efficacy of transcatheter aortic valve implantation in low-risk patients.
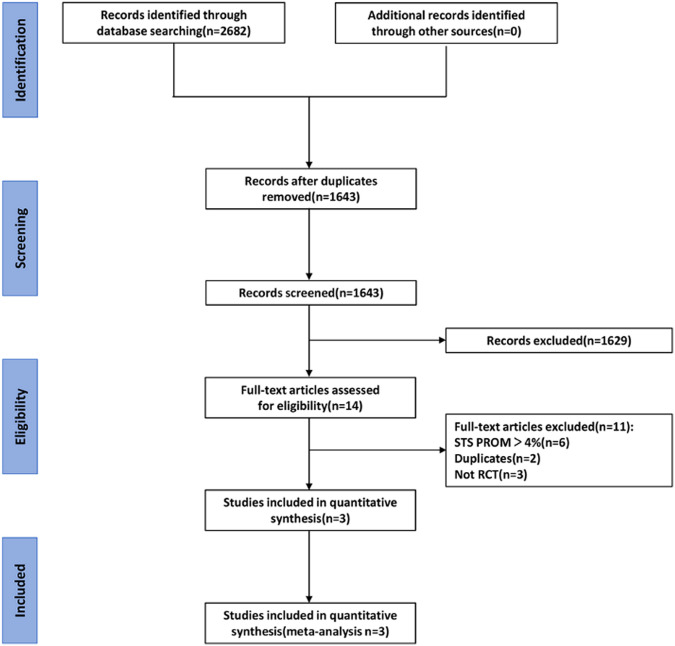
From the outset of our initiative until April 2022, PubMed, EMBASE, and the Cochrane database were thoroughly searched, yielding the selection of 3 randomized controlled trials including 2644 patients with aortic stenosis, to assess outcome measures at distinct follow-up time.
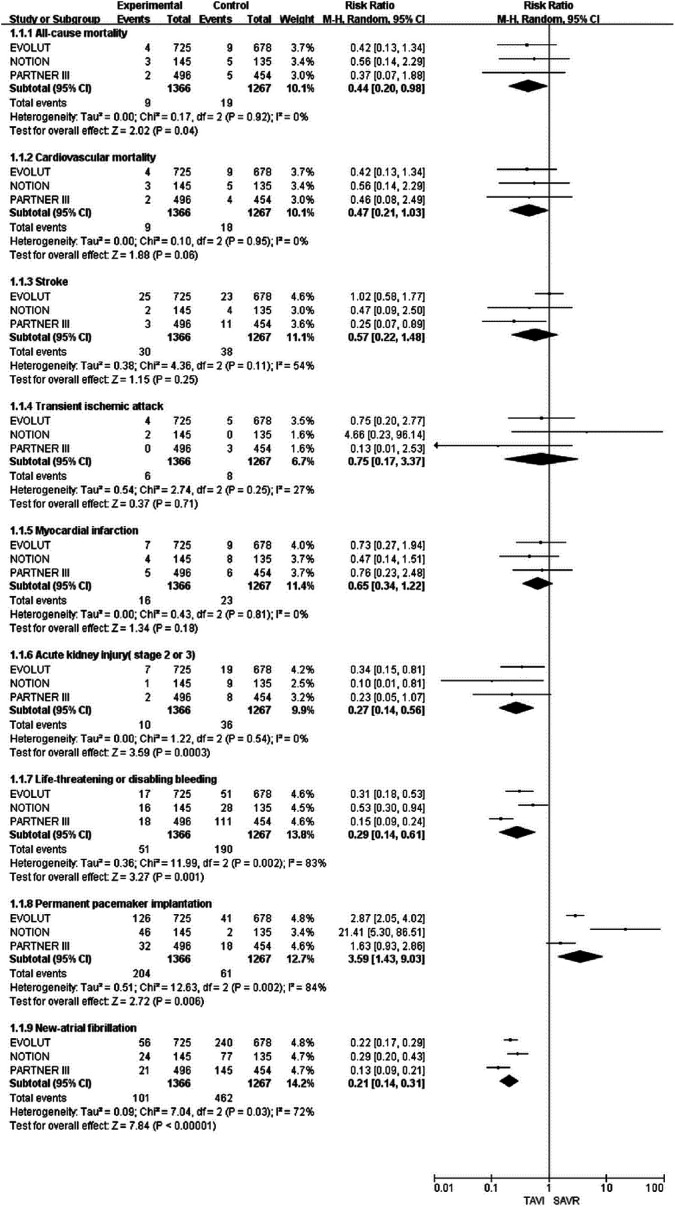
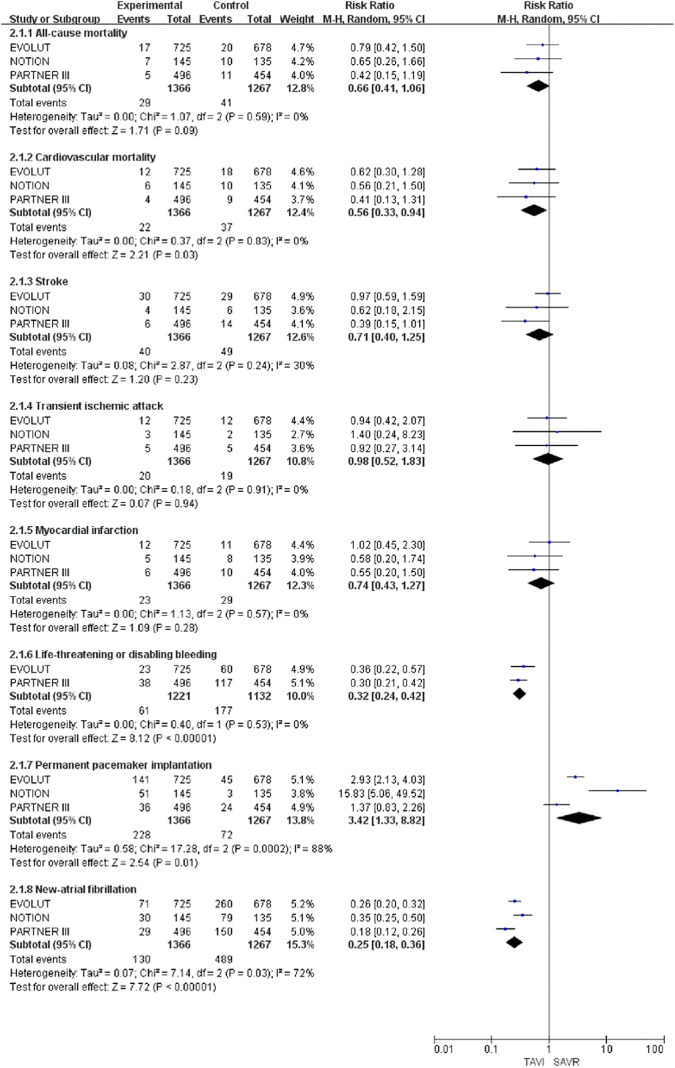
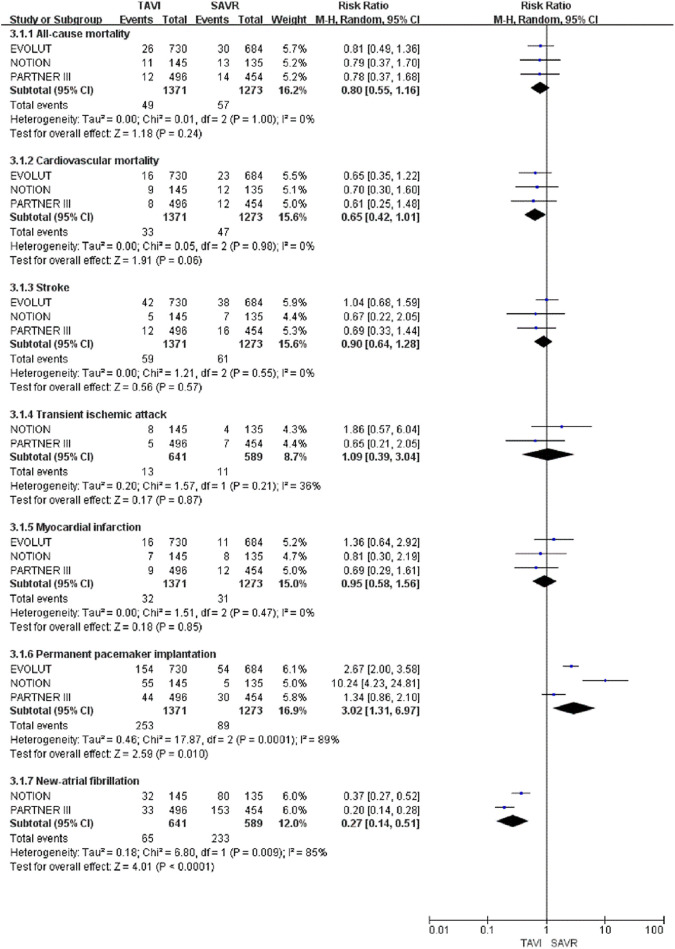
The mean Society of Thoracic Surgeons Predicted Risk of Mortality score of patients was 2.2. At the 30-day and 1-year follow-up, transcatheter aortic valve implan- tation was associated with a lower incidence of all-cause mortality, cardiovascular mor- tality, acute kidney injury (stage 2 or 3), life-threatening or significant bleeding, and new atrial fibrillation but an increased risk of permanent pacemaker implantation. At the 2-year follow-up, transcatheter aortic valve implantation only had an advantage in new atrial fibrillation (relative risk, 0.27; 95% CI, 0.14-0.51; P < .0001), with no significant differ- ence in all-cause mortality or cardiovascular mortality.
For low-risk surgical patients with aortic stenosis, compared to surgical aortic valve replacement, transcatheter aortic valve implantation was associated with lower all-cause mortality at 30-day follow-up and lower cardiovascular mortality at 1-year follow-up. Except for the advantages in new atrial fibrillation, transcatheter aor- tic valve implantation had no significant impact on mortality at 2-year follow-up.
先前的研究表明,对于高危外科主动脉瓣狭窄患者,经导管主动脉瓣植入术是外科主动脉瓣置换术的最佳替代治疗方法。然而,目前尚不清楚经导管主动脉瓣植入术是否可用于低危外科主动脉瓣狭窄患者。本研究旨在评估经导管主动脉瓣植入术在低危患者中的安全性和疗效。
从我们的研究开始到 2022 年 4 月,我们彻底检索了 PubMed、EMBASE 和 Cochrane 数据库,共纳入了 3 项随机对照试验,包括 2644 例主动脉瓣狭窄患者,以评估不同随访时间的结局指标。
患者的平均胸外科医师协会预测死亡率评分(Society of Thoracic Surgeons Predicted Risk of Mortality score)为 2.2。在 30 天和 1 年随访时,经导管主动脉瓣植入术与全因死亡率、心血管死亡率、急性肾损伤(第 2 或 3 阶段)、危及生命或显著出血和新发心房颤动发生率降低相关,但与永久性心脏起搏器植入风险增加相关。在 2 年随访时,经导管主动脉瓣植入术仅在新发心房颤动方面具有优势(相对风险,0.27;95%置信区间,0.14-0.51;P <.0001),而全因死亡率或心血管死亡率无显著差异。
对于低危外科主动脉瓣狭窄患者,与外科主动脉瓣置换术相比,经导管主动脉瓣植入术在 30 天随访时全因死亡率较低,在 1 年随访时心血管死亡率较低。除新发心房颤动方面的优势外,经导管主动脉瓣植入术在 2 年随访时对死亡率无显著影响。