Department of Radiation Oncology, Stanford University, Palo Alto, California.
Palo Alto Veterans Affairs Hospital, Palo Alto, California.
JAMA Netw Open. 2022 Aug 1;5(8):e2226327. doi: 10.1001/jamanetworkopen.2022.26327.
Improper aggregation of Native Hawaiian and other Pacific Islander individuals with Asian individuals can mask Native Hawaiian and other Pacific Islander patient outcomes. A comprehensive assessment of cancer disparities comparing Asian with Native Hawaiian and other Pacific Islander populations is lacking.
To compare comorbidity burden and survival among East Asian, Native Hawaiian and other Pacific Islander, South Asian, and Southeast Asian individuals with non-Hispanic White individuals with cancer.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study used a national hospital-based oncology database enriched with Native Hawaiian and other Pacific Islander and Asian populations. Asian, Native Hawaiian and other Pacific Islander, and White individuals diagnosed with the most common cancers who received treatment from January 1, 2004, to December 31, 2017, were included. Patients younger than 18 years, without pathologic confirmation of cancer, or with metastatic disease were excluded. Data were analyzed from January to May 2022.
The primary end points were comorbidity burden by Charlson-Deyo Comorbidity Index and overall survival (OS).
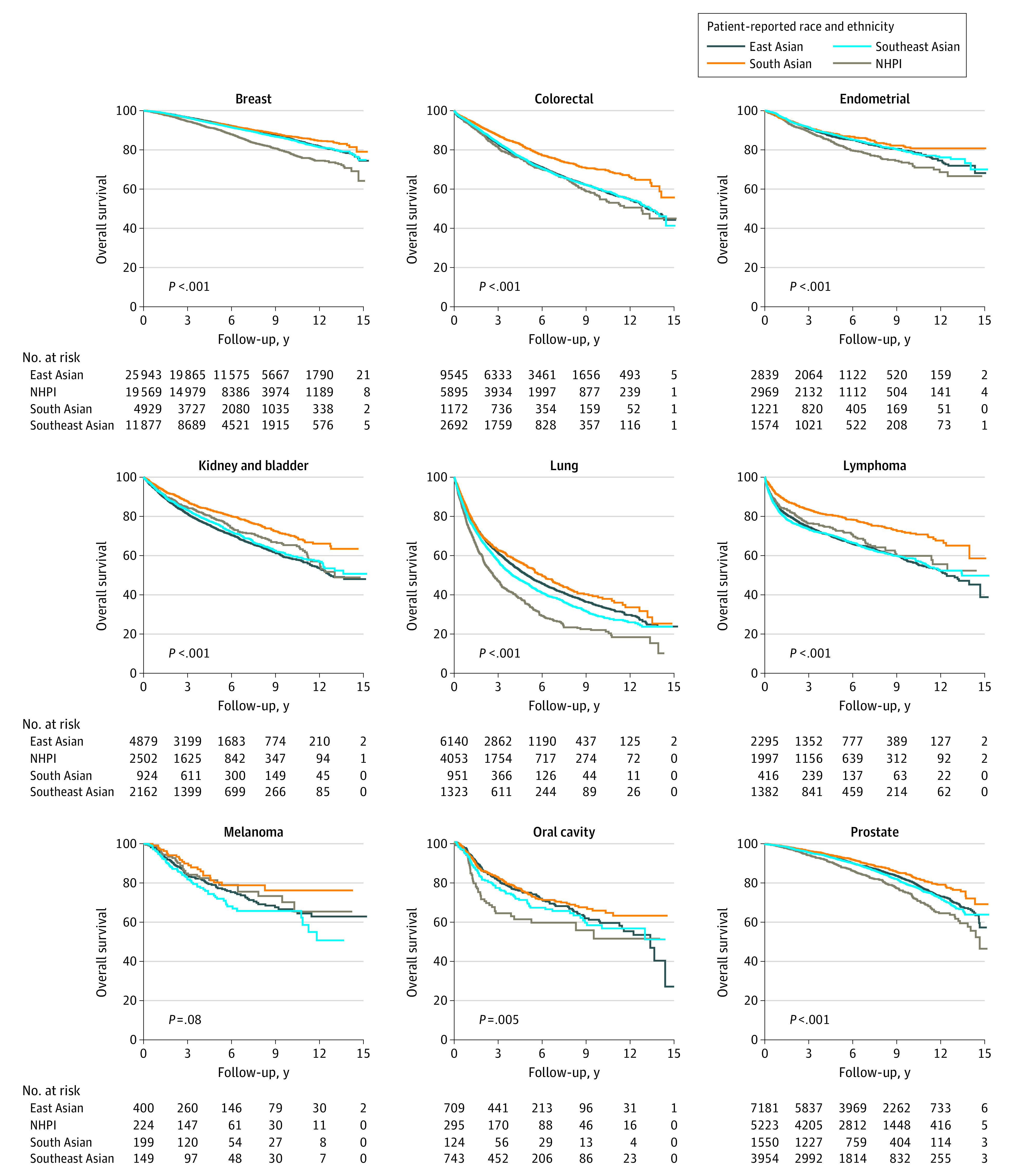
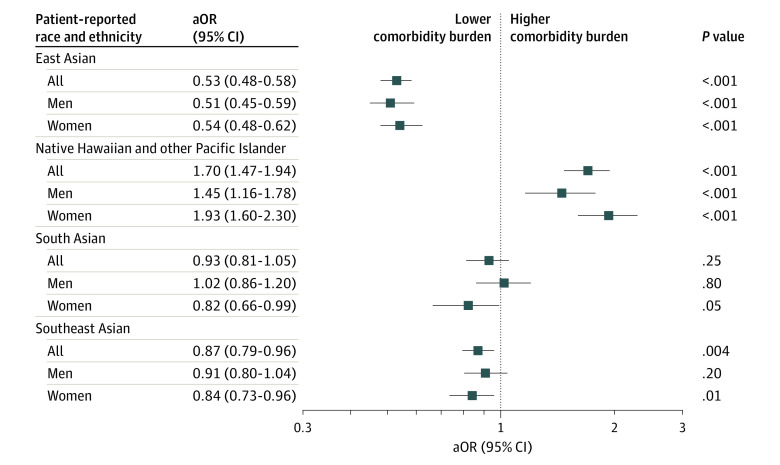
In total, 5 955 550 patients were assessed, including 60 047 East Asian, 11 512 Native Hawaiian and other Pacific Islander, 25 966 South Asian, 42 815 Southeast Asian, and 5 815 210 White patients. The median (IQR) age was 65 (56-74) years, median (IQR) follow-up was 58 (30-96) months, and 3 384 960 (57%) were women. Patients were predominantly from metropolitan areas (4 834 457 patients [84%]) and the Southern United States (1 987 506 patients [34%]), with above median education (3 576 460 patients [65%]), and without comorbidities (4 603 386 patients [77%]). Cancers included breast (1 895 351 patients [32%]), prostate (948 583 patients [16%]), kidney or bladder (689 187 patients [12%]), lung (665 622 patients [11%]), colorectal (659 165 patients [11%]), melanoma (459 904 patients [8%]), endometrial (307 401 patients [5%]), lymphoma (245 003 patients [4%]), and oral cavity (85 334 patients [1%]) malignant neoplasms. Native Hawaiian and other Pacific Islander patients had the highest comorbidity burden (adjusted odds ratio [aOR], 1.70; 95% CI, 1.47-1.94) compared with Asian and White groups. Asian patients had superior OS compared with White patients for most cancers; only Southeast Asian patients with lymphoma had inferior survival (adjusted hazard ratio [aHR], 1.26; 95% CI, 1.16-1.37). In contrast, Native Hawaiian and other Pacific Islander patients demonstrated inferior OS compared with Asian and White patients for oral cavity cancer (aHR, 1.56; 95% CI, 1.14-2.13), lymphoma (aHR, 1.35; 95% CI, 1.11-1.63), endometrial cancer (aHR, 1.30; 95% CI, 1.12-1.50), prostate cancer (aHR, 1.29; 95% CI, 1.14-1.46), and breast cancer (aHR, 1.09; 95% CI, 1.00-1.18). No cancers among Native Hawaiian and other Pacific Islander patients had superior OS compared with White patients.
In this cohort study, compared with White patients with the most common cancers, Asian patients had superior survival outcomes while Native Hawaiian and other Pacific Islander patients had inferior survival outcomes. Native Hawaiian and other Pacific Islander patients had significantly greater comorbidity burden compared with Asian and White patients, but this alone did not explain the poor survival outcomes. These results support the disaggregation of these groups in cancer studies.
不恰当地将夏威夷原住民和其他太平洋岛民个体与亚洲个体进行合并,可能会掩盖夏威夷原住民和其他太平洋岛民患者的结局。缺乏对亚洲人、夏威夷原住民和其他太平洋岛民与南亚人、东南亚人癌症差异的全面评估。
比较非西班牙裔白种人与亚洲人(包括东亚人、夏威夷原住民和其他太平洋岛民、南亚人和东南亚人)的合并症负担和生存情况。
设计、设置和参与者:这是一项回顾性队列研究,使用了一个全国性的医院肿瘤数据库,该数据库丰富了夏威夷原住民和其他太平洋岛民以及亚洲人群的数据。纳入了从 2004 年 1 月 1 日至 2017 年 12 月 31 日期间接受治疗、诊断出最常见癌症且年龄在 18 岁以下、无癌症病理确认或患有转移性疾病的非西班牙裔白种人、亚洲人、夏威夷原住民和其他太平洋岛民和白种人患者。数据于 2022 年 1 月至 5 月进行分析。
主要终点是 Charlson-Deyo 合并症指数评估的合并症负担和总生存(OS)。
共评估了 5955550 名患者,包括 60047 名东亚人、11512 名夏威夷原住民和其他太平洋岛民、25966 名南亚人、42815 名东南亚人和 5815210 名白种人。患者的中位(IQR)年龄为 65(56-74)岁,中位(IQR)随访时间为 58(30-96)个月,3384960 名(57%)为女性。患者主要来自大都市区(4834457 名[84%])和美国南部(1987506 名[34%]),受教育程度较高(3576460 名[65%]),无合并症(4603386 名[77%])。癌症包括乳腺癌(1895351 名患者[32%])、前列腺癌(948583 名患者[16%])、肾或膀胱癌(689187 名患者[12%])、肺癌(665622 名患者[11%])、结直肠癌(659165 名患者[11%])、黑色素瘤(459904 名患者[8%])、子宫内膜癌(307401 名患者[5%])、淋巴瘤(245003 名患者[4%])和口腔癌(85334 名患者[1%])恶性肿瘤。与亚洲人和白种人相比,夏威夷原住民和其他太平洋岛民患者的合并症负担最高(调整优势比[aOR],1.70;95%CI,1.47-1.94)。对于大多数癌症,亚洲患者的 OS 优于白种人;只有东南亚淋巴瘤患者的生存率较低(调整后的危险比[aHR],1.26;95%CI,1.16-1.37)。相比之下,夏威夷原住民和其他太平洋岛民患者的口腔癌(aHR,1.56;95%CI,1.14-2.13)、淋巴瘤(aHR,1.35;95%CI,1.11-1.63)、子宫内膜癌(aHR,1.30;95%CI,1.12-1.50)、前列腺癌(aHR,1.29;95%CI,1.14-1.46)和乳腺癌(aHR,1.09;95%CI,1.00-1.18)的 OS 均劣于亚洲人和白种人。与白种人相比,夏威夷原住民和其他太平洋岛民患者没有任何癌症的 OS 更好。
在这项队列研究中,与患有最常见癌症的白种人相比,亚洲患者的生存结果更好,而夏威夷原住民和其他太平洋岛民患者的生存结果更差。与亚洲人和白种人相比,夏威夷原住民和其他太平洋岛民患者的合并症负担明显更大,但这并不能完全解释其较差的生存结果。这些结果支持在癌症研究中对这些群体进行细分。