Division of Trauma and Emergency Surgery, Department of Surgery, Chang Gung Memorial Hospital, Chang Gung University, 5, Fu-Hsing Street, Kwei-Shan, Tao-Yuan City, 333, Taiwan.
Division of Emergency and Critical Care Radiology, Department of Medical Imaging and Intervention, Chang Gung Memorial Hospital, Chang Gung University, Tao-Yuan City, Taiwan.
Surg Endosc. 2023 Jan;37(1):371-381. doi: 10.1007/s00464-022-09531-0. Epub 2022 Aug 12.
This study aimed to evaluate the management of blunt splenic injury (BSI) and highlight the role of splenic artery embolization (SAE).
We conducted a retrospective review of all patients with BSI over 15 years. Splenic injuries were graded by the 2018 revision of the American Association for the Surgery of Trauma-Organ Injury Scale (AAST-OIS). Our hospital provide 24/7 in-house surgeries and 24/7 in-house interventional radiology facility. Patients with BSI who arrived hypotensive and were refractory to resuscitation required surgery and patients with vascular injury on abdominal computed tomography were considered for SAE.
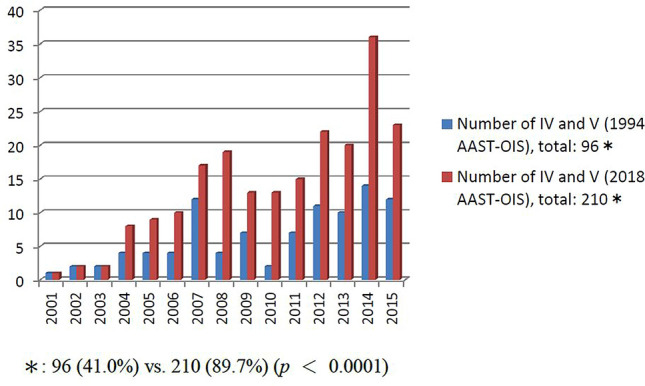
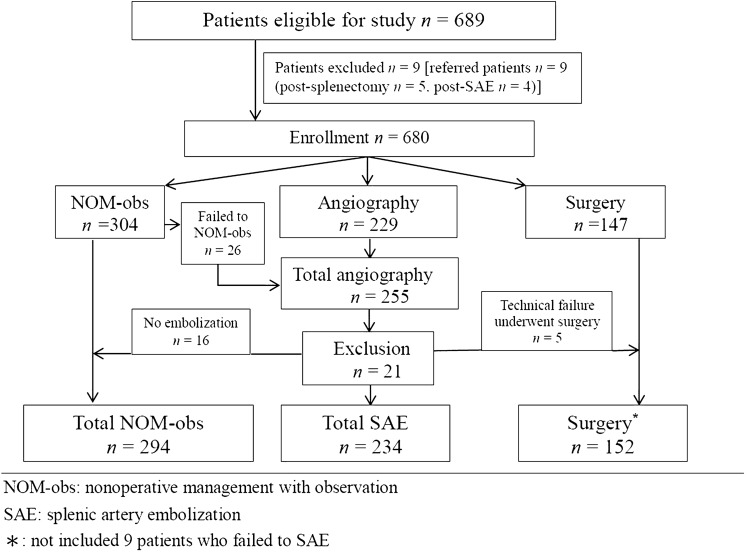
In total, 680 patients with BSI, the number of patients who underwent nonoperative management with observation (NOM-obs), SAE, and surgery was 294, 234, and 152, respectively. The number of SAEs increased from 4 (8.3%) in 2001 to 23 (60.5%) in 2015 (p < 0.0001); conversely, the number of surgeries decreased from 21 (43.8%) in 2001 to 4 (10.5%) in 2015 (p = 0.001). The spleen-related mortality rate of NOM-obs, SAEs, and surgery was 0%, 0.4%, and 7.2%, respectively. In the SAE subgroup, according to the 2018 AAST-OIS, 234 patients were classified as grade II, n = 3; III, n = 21; IV, n = 111; and V, n = 99, respectively.; and compared with 1994 AST-OIS, 150 patients received a higher grade and the total number of grade IV and V injuries ranged from 96 (41.0%) to 210 (89.7%) (p < 0.0001). On angiography, 202 patients who demonstrated vascular injury and 187 achieved hemostasis after SAE with a 92.6% success rate. Six of the 15 patients failed to SAE preserved the spleen after second embolization with a 95.5% salvage rate.
Our data confirm the superiority of the 2018 AAST-OIS and support the role of SAE in changing the trend of management of BSI.
本研究旨在评估钝性脾损伤(BSI)的处理方法,并强调脾动脉栓塞术(SAE)的作用。
我们对 15 年来所有 BSI 患者进行了回顾性研究。脾损伤按 2018 年美国创伤外科学会-器官损伤分级标准(AAST-OIS)进行分级。我们医院提供 24/7 院内手术和 24/7 院内介入放射学设施。入院时低血压且复苏无效的 BSI 患者需要手术,腹部计算机断层扫描显示血管损伤的患者需要考虑 SAE。
共有 680 例 BSI 患者,分别接受非手术治疗观察(NOM-obs)、SAE 和手术治疗的患者有 294 例、234 例和 152 例。SAE 的数量从 2001 年的 4 例(8.3%)增加到 2015 年的 23 例(60.5%)(p<0.0001);相反,手术的数量从 2001 年的 21 例(43.8%)减少到 2015 年的 4 例(10.5%)(p=0.001)。NOM-obs、SAE 和手术的脾相关死亡率分别为 0%、0.4%和 7.2%。在 SAE 亚组中,根据 2018 年 AAST-OIS,234 例患者分别被归类为 II 级,n=3;III 级,n=21;IV 级,n=111;V 级,n=99;与 1994 年 AAST-OIS 相比,150 例患者获得了更高的等级,IV 级和 V 级损伤的总数从 96 例(41.0%)增加到 210 例(89.7%)(p<0.0001)。血管造影显示,202 例有血管损伤的患者和 187 例患者在 SAE 后达到止血,成功率为 92.6%。在未能进行 SAE 的 15 例患者中,有 6 例在第二次栓塞后保留了脾脏,保脾成功率为 95.5%。
我们的数据证实了 2018 年 AAST-OIS 的优越性,并支持 SAE 在改变 BSI 处理趋势方面的作用。