Kidney Transplant Unit, Nephrology Department. Montpellier University Hospital, Montpellier, France.
Kidney transplant Unit. Nephrology Department. Vall d'Hebron Hospital Universitari, Vall d'Hebron Institut de Recerca (VHIR), Universitat Autònoma de Barcelona, Barcelona, Spain.
Front Immunol. 2022 Jul 29;13:918887. doi: 10.3389/fimmu.2022.918887. eCollection 2022.
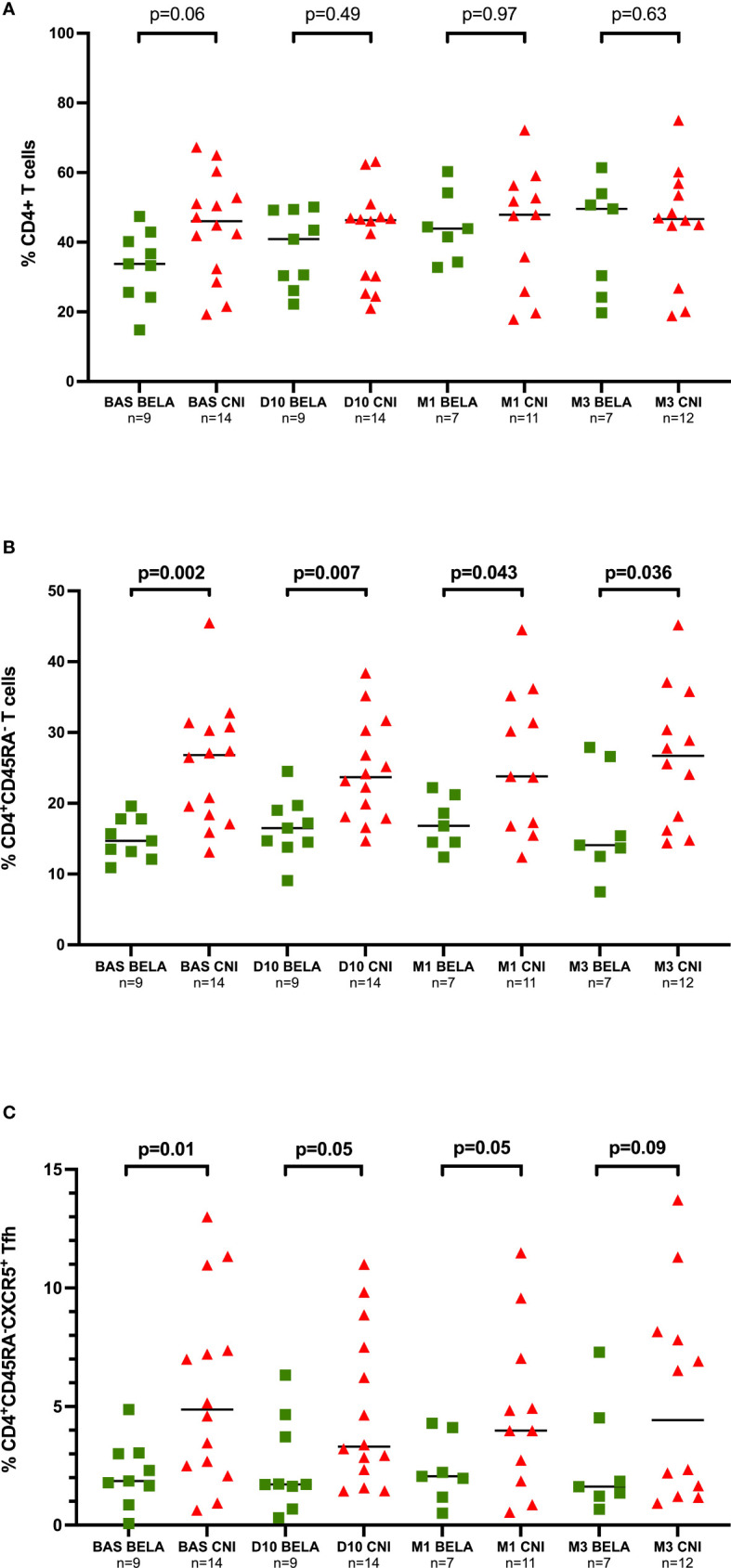
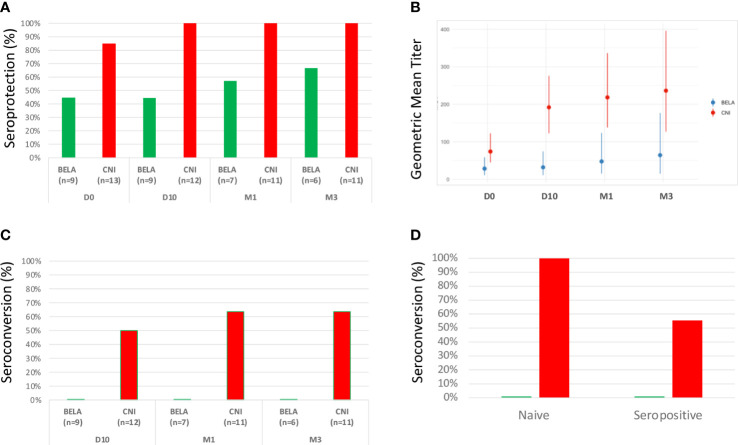
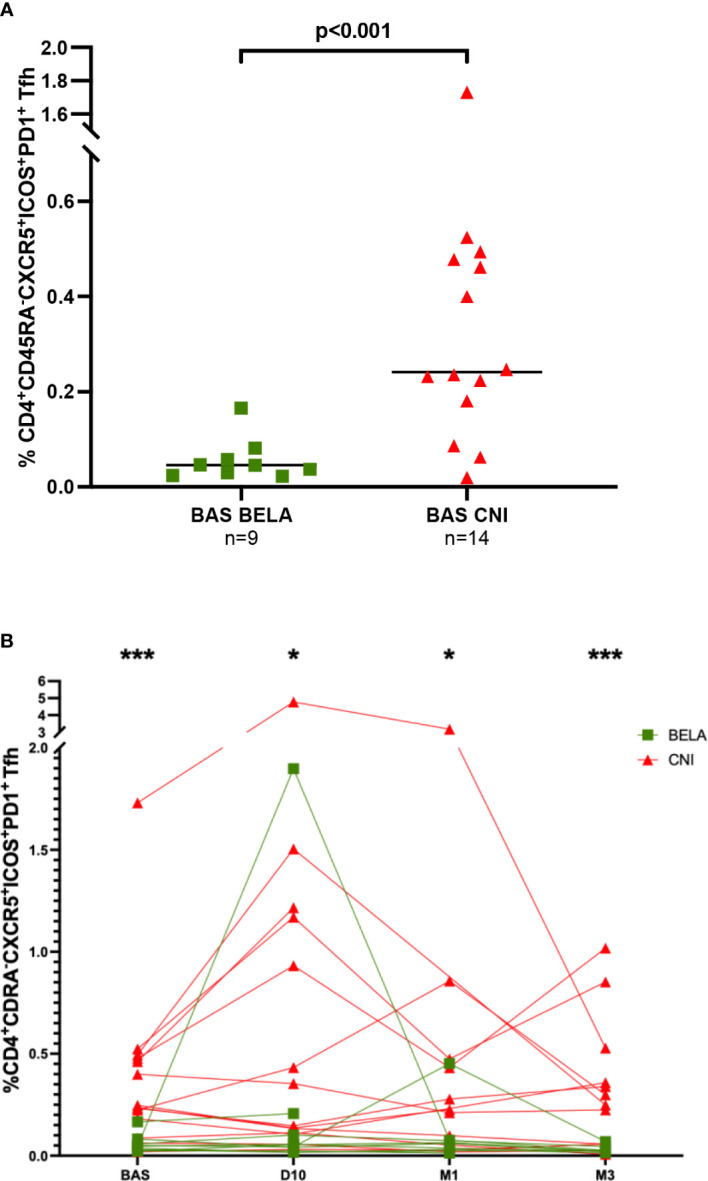
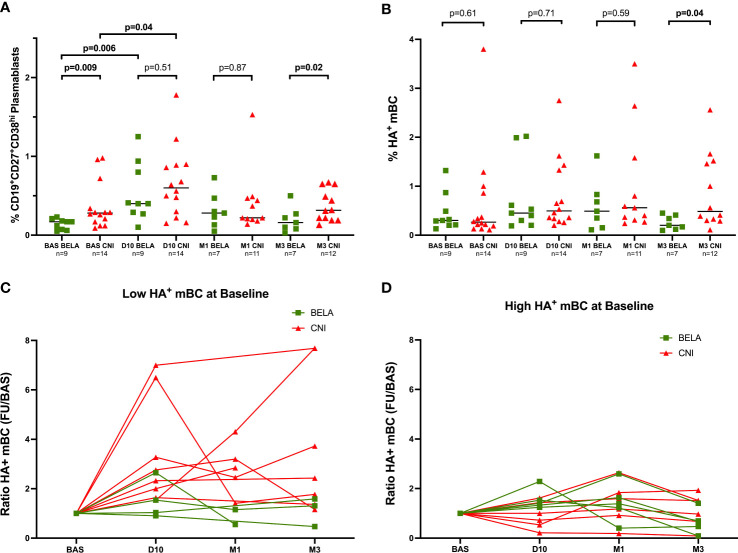
Emerging data suggest that costimulation blockade with belatacept effectively controls humoral alloimmune responses. However, whether this effect may be deleterious for protective anti-infectious immunity remains poorly understood. We performed a mechanistic exploratory study in 23 kidney transplant recipients receiving either the calcineurin-inhibitor tacrolimus (Tac, n=14) or belatacept (n=9) evaluating different cellular immune responses after influenza vaccination such as activated T follicular Helper (Tfh), plasmablasts and H1N1 hemagglutinin (HA)-specific memory B cells (HAmBC) by flow-cytometry, and anti-influenza antibodies by hemagglutination inhibition test (HI), at baseline and days 10, 30 and 90 post-vaccination. The proportion of CD4+CD54RA-CXCR5+ Tfh was lower in belatacept than Tac patients at baseline (1.86%[1.25-3.03] 4.88%[2.40-8.27], p=0.01) and remained stable post-vaccination. At M3, HAmBc were significantly higher in Tac-treated patients (0.56%[0.32-1.49] 0.27%[0.13-0.44], p=0.04) and correlated with activated Tfh numbers. When stratifying patients according to baseline HAmBc frequencies, belatacept patients with low HAmBC displayed significantly lower HAmBc increases after vaccination than Tac patients (1.28[0.94-2.4] 2.54[1.73-5.70], p=0.04). Also, belatacept patients displayed significantly lower seroprotection rates against H1N1 at baseline than Tac-treated patients (44.4% 84.6%) as well as lower seroconversion rates at days 10, 30 and 90 after vaccination (50% 0%, 63.6% 0%, and 63.6% 0%, respectively). We show the efficacy of belatacept inhibiting T-dependent antigen-specific humoral immune responses, active immunization should be highly encouraged before starting belatacept therapy.
新兴数据表明,使用贝利尤单抗进行共刺激阻断可有效控制体液性同种异体免疫反应。然而,对于保护性抗感染免疫,这种效果是否有害仍知之甚少。我们在 23 名接受钙调神经磷酸酶抑制剂他克莫司(Tac,n=14)或贝利尤单抗(n=9)治疗的肾移植受者中进行了一项机制探索性研究,通过流式细胞术评估了流感疫苗接种后不同的细胞免疫反应,如活化滤泡辅助 T 细胞(Tfh)、浆母细胞和 H1N1 血凝素(HA)特异性记忆 B 细胞(HAmBC),并通过血凝抑制试验(HI)评估了抗流感抗体,在基线和接种后 10、30 和 90 天进行评估。与 Tac 组相比,贝利尤单抗组患者基线时 CD4+CD54RA-CXCR5+Tfh 比例较低(1.86%[1.25-3.03] 4.88%[2.40-8.27],p=0.01),接种后仍保持稳定。在 M3 时,Tac 组患者的 HAmBc 明显更高(0.56%[0.32-1.49] 0.27%[0.13-0.44],p=0.04),且与活化 Tfh 数量相关。当根据基线 HAmBc 频率对患者进行分层时,基线 HAmBC 较低的贝利尤单抗组患者接种后 HAmBc 增加幅度明显低于 Tac 组(1.28%[0.94-2.4] 2.54%[1.73-5.70],p=0.04)。此外,与 Tac 治疗组相比,贝利尤单抗组患者的基线 H1N1 血清保护率显著较低(44.4% 84.6%),且接种后 10、30 和 90 天时的血清转化率也较低(50% 0%,63.6% 0%和 63.6% 0%)。我们证明了贝利尤单抗抑制 T 依赖性抗原特异性体液免疫反应的疗效,在开始贝利尤单抗治疗前应强烈鼓励进行主动免疫接种。