Steno Diabetes Center Copenhagen, Herlev, Denmark.
Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark.
Diabetes Care. 2022 Dec 1;45(12):2991-2998. doi: 10.2337/dc22-0294.
Finerenone reduced the risk of kidney and cardiovascular events in people with chronic kidney disease (CKD) and type 2 diabetes in the FIDELIO-DKD and FIGARO-DKD phase 3 studies. Effects of finerenone on outcomes in patients taking sodium-glucose cotransporter 2 inhibitors (SGLT2is) were evaluated in a prespecified pooled analysis of these studies.
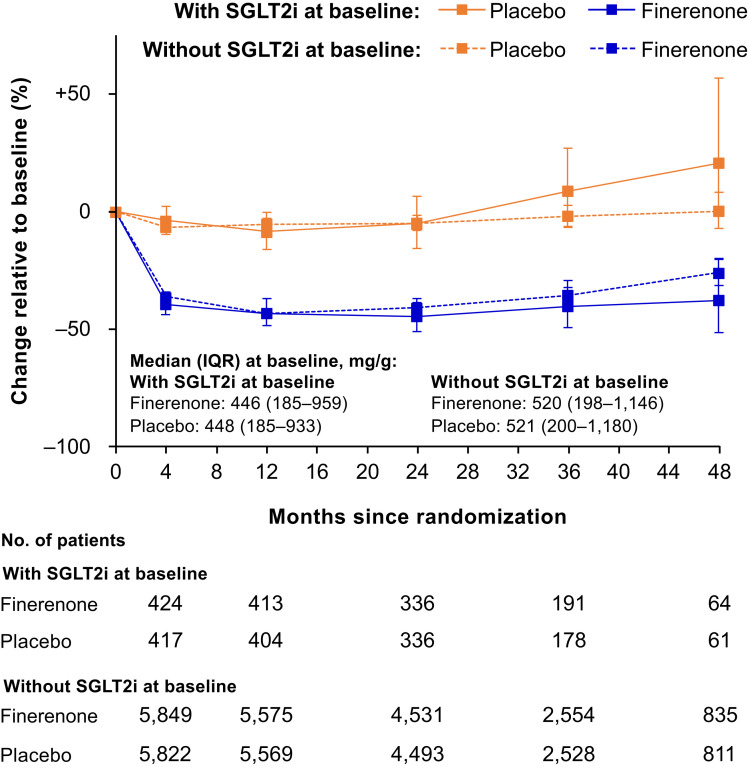
Patients with type 2 diabetes and urine albumin-to-creatinine ratio (UACR) ≥30 to ≤5,000 mg/g and estimated glomerular filtration rate (eGFR) ≥25 mL/min/1.73 m2 were randomly assigned to finerenone or placebo; SGLT2is were permitted at any time. Outcomes included cardiovascular composite (cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure) and kidney composite (kidney failure, sustained ≥57% eGFR decline, or renal death) end points, changes in UACR and eGFR, and safety outcomes.
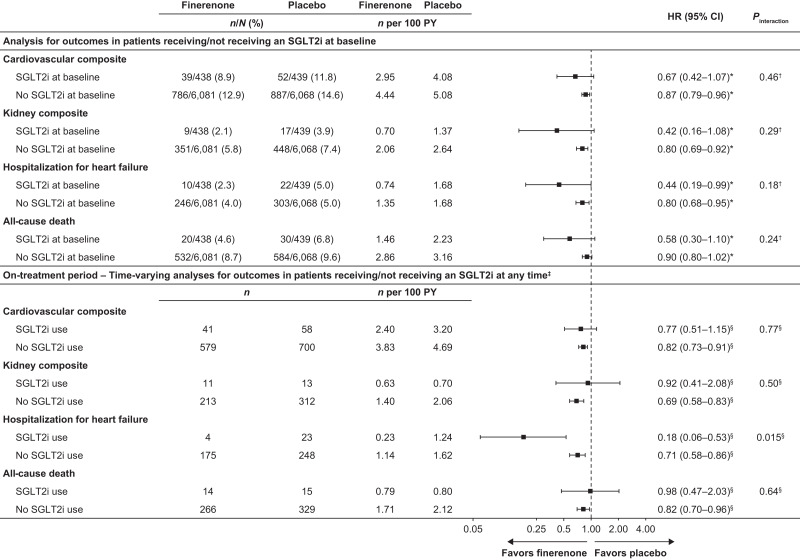
Among 13,026 patients, 877 (6.7%) received an SGLT2i at baseline and 1,113 (8.5%) initiated one during the trial. For the cardiovascular composite, the hazard ratios (HRs) were 0.87 (95% CI 0.79-0.96) without SGLT2i and 0.67 (95% CI 0.42-1.07) with SGLT2i. For the kidney composite, the HRs were 0.80 (95% CI 0.69-0.92) without SGLT2i and 0.42 (95% CI 0.16-1.08) with SGLT2i. Baseline SGLT2i use did not affect risk reduction for the cardiovascular or kidney composites with finerenone (Pinteraction = 0.46 and 0.29, respectively); neither did SGLT2i use concomitant with study treatment.
Benefits of finerenone compared with placebo on cardiorenal outcomes in patients with CKD and type 2 diabetes were observed irrespective of SGLT2i use.
非奈利酮可降低慢性肾脏病(CKD)和 2 型糖尿病患者的肾脏和心血管事件风险,这在 FIDELIO-DKD 和 FIGARO-DKD 这两项 3 期研究中得到了证实。在这两项研究的预设汇总分析中,评估了非奈利酮对接受钠-葡萄糖共转运蛋白 2 抑制剂(SGLT2i)治疗的患者的结局影响。
纳入 UACR(尿白蛋白与肌酐比值)≥30 至 ≤5000mg/g 且估算肾小球滤过率(eGFR)≥25ml/min/1.73m2 的 2 型糖尿病患者,随机分配至非奈利酮或安慰剂组;任何时间都允许使用 SGLT2i。主要终点为心血管复合终点(心血管死亡、非致死性心肌梗死、非致死性卒中和因心力衰竭住院)和肾脏复合终点(肾衰竭、持续 eGFR 下降≥57%或肾脏死亡),以及 UACR 和 eGFR 的变化和安全性结局。
在 13026 例患者中,877 例(6.7%)基线时接受 SGLT2i 治疗,1113 例(8.5%)在试验期间开始使用 SGLT2i。无 SGLT2i 治疗时,心血管复合终点的 HR 为 0.87(95%CI,0.79-0.96),有 SGLT2i 治疗时为 0.67(95%CI,0.42-1.07)。无 SGLT2i 治疗时,肾脏复合终点的 HR 为 0.80(95%CI,0.69-0.92),有 SGLT2i 治疗时为 0.42(95%CI,0.16-1.08)。基线时使用 SGLT2i 不影响非奈利酮治疗的患者的心血管或肾脏复合终点的风险降低(P 交互作用=0.46 和 0.29);同时使用 SGLT2i 与研究治疗也不影响。
无论是否使用 SGLT2i,非奈利酮与安慰剂相比,都可降低 CKD 和 2 型糖尿病患者的心脏肾脏结局风险。