Department of Surgery, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire.
Geisel School of Medicine at Dartmouth, Hanover, New Hampshire.
JAMA Health Forum. 2021 Sep 3;2(9):e212324. doi: 10.1001/jamahealthforum.2021.2324. eCollection 2021 Sep.
Treatment delays are associated with increased morbidity and cost of disease, although the extent to which cost sharing influences timely presentation and management of acute surgical disease remains unknown. Given recent policy changes using cost sharing to modify health care behavior, this study examines the association of cost sharing with the health of the patient at presentation and with receipt of optimal or minimally invasive surgery.
To assess whether cost sharing is associated with the likelihood of early, uncomplicated patient presentation or with surgical management of 2 representative emergency general surgery diagnoses: acute appendicitis and acute diverticulitis.
This cohort study used Health Care Cost Institute claims from January 1, 2013, through December 31, 2017, to analyze data of commercially insured individuals hospitalized for acute appendicitis or diverticulitis. In total, 151 852 patients in the data set aged 18 to 64 years and presenting with acute appendicitis or diverticulitis were included as identified using the and the . Data were analyzed from January 2020 through February 2021.
The primary exposure was patient total cost sharing incurred for the index hospitalization, defined as their summed deductible, copayments, and coinsurance.
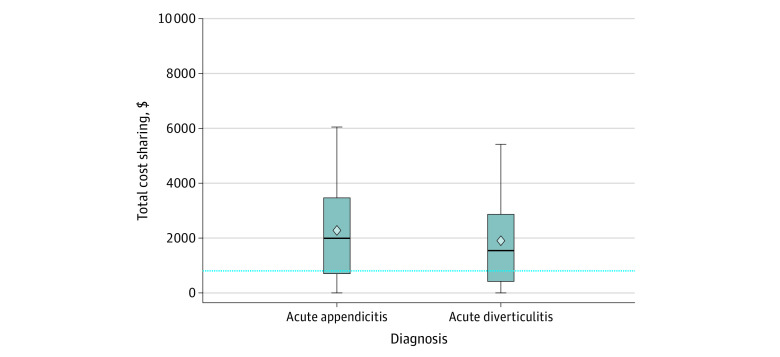
The primary outcome was early, uncomplicated disease presentation. Secondary outcomes were receipt of optimal surgical care and minimally invasive surgery if undergoing an operation. Analyses were conducted with multivariable logistic regression models to adjust for patient characteristics and community-level socioeconomic and geographic factors. High cost sharing was defined as quartile 4 (>$3082), and low cost sharing as quartile 1 ($0-$502).
Among 151 852 patients, 52.4% were men, and the total cost-sharing median was $1725 (interquartile range, $503-$3082). Higher cost sharing was associated with lower odds of early, uncomplicated disease presentation (odds ratio, 0.63; 95% CI, 0.61-0.65). Patients with higher cost sharing were less likely to receive optimal surgical care (odds ratio, 0.96; 95% CI, 0.93-0.99) or minimally invasive surgery (odds ratio, 0.89; 95% CI, 0.84-0.95).
The findings of this cohort study suggest that, as policymakers debate the degree of cost sharing in public and private insurance plans, attention should be given to the clinical and financial implications associated with care delays.
治疗延误与疾病发病率和成本增加有关,尽管成本分担在多大程度上影响急性外科疾病的及时就诊和管理尚不清楚。鉴于最近使用成本分担来改变医疗行为的政策变化,本研究调查了成本分担与患者就诊时的健康状况以及是否接受最佳或微创手术之间的关系。
评估成本分担是否与早期、无并发症的患者就诊或 2 种代表性的急诊普通外科诊断(急性阑尾炎和急性憩室炎)的手术管理相关。
设计、设置和参与者:这项队列研究使用了 2013 年 1 月 1 日至 2017 年 12 月 31 日期间的健康成本研究所索赔数据,对因急性阑尾炎或憩室炎住院的商业保险个人的数据进行了分析。在数据集中,共有 151852 名年龄在 18 至 64 岁之间的患者被确定为患有急性阑尾炎或憩室炎,他们是使用 和 确定的。数据分析于 2020 年 1 月至 2021 年 2 月进行。
主要暴露因素是患者因指数住院而产生的总自付费用,定义为他们的免赔额、共同支付额和自付额总和。
主要结果是早期、无并发症的疾病表现。次要结果是接受最佳手术护理和接受手术时的微创手术。使用多变量逻辑回归模型进行分析,以调整患者特征和社区层面的社会经济和地理因素。高成本分担被定义为第 4 四分位数(>$3082),低成本分担被定义为第 1 四分位数($0-$502)。
在 151852 名患者中,52.4%为男性,总成本分担中位数为 1725 美元(四分位距,503-3082 美元)。较高的成本分担与早期、无并发症疾病表现的可能性降低相关(比值比,0.63;95%CI,0.61-0.65)。成本分担较高的患者不太可能接受最佳手术护理(比值比,0.96;95%CI,0.93-0.99)或微创手术(比值比,0.89;95%CI,0.84-0.95)。
这项队列研究的结果表明,在政策制定者就公共和私人保险计划中的成本分担程度进行辩论时,应关注与护理延误相关的临床和财务影响。