Division of Research, Kaiser Permanente, Oakland, California.
The Permanente Medical Group, Oakland, California.
JAMA Health Forum. 2021 Aug 20;2(8):e212095. doi: 10.1001/jamahealthforum.2021.2095. eCollection 2021 Aug.
Identifying the most efficient COVID-19 vaccine allocation strategy may substantially reduce hospitalizations and save lives while ensuring an equitable vaccine distribution.
To simulate the association of different vaccine allocation strategies with COVID-19-associated morbidity and mortality and their distribution across racial and ethnic groups.
We developed and internally validated the risk of COVID-19 infection and risk of hospitalization models on randomly split training and validation data sets. These were used in a computer simulation study of vaccine prioritization among adult health plan members who were drawn from an integrated health care delivery system. The study was conducted from January 3, 2021, to June 1, 2021, in Oakland, California, and the data were analyzed during the same period.
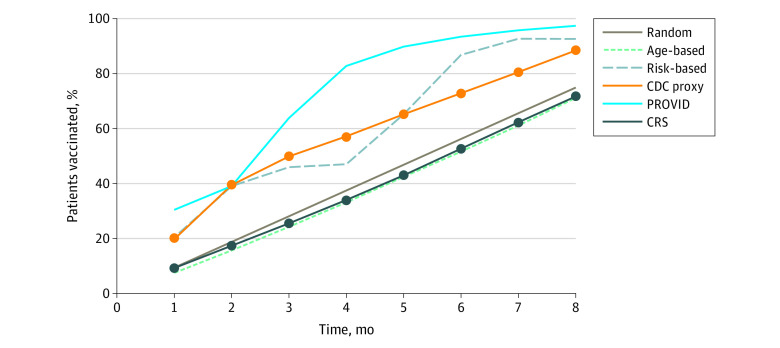
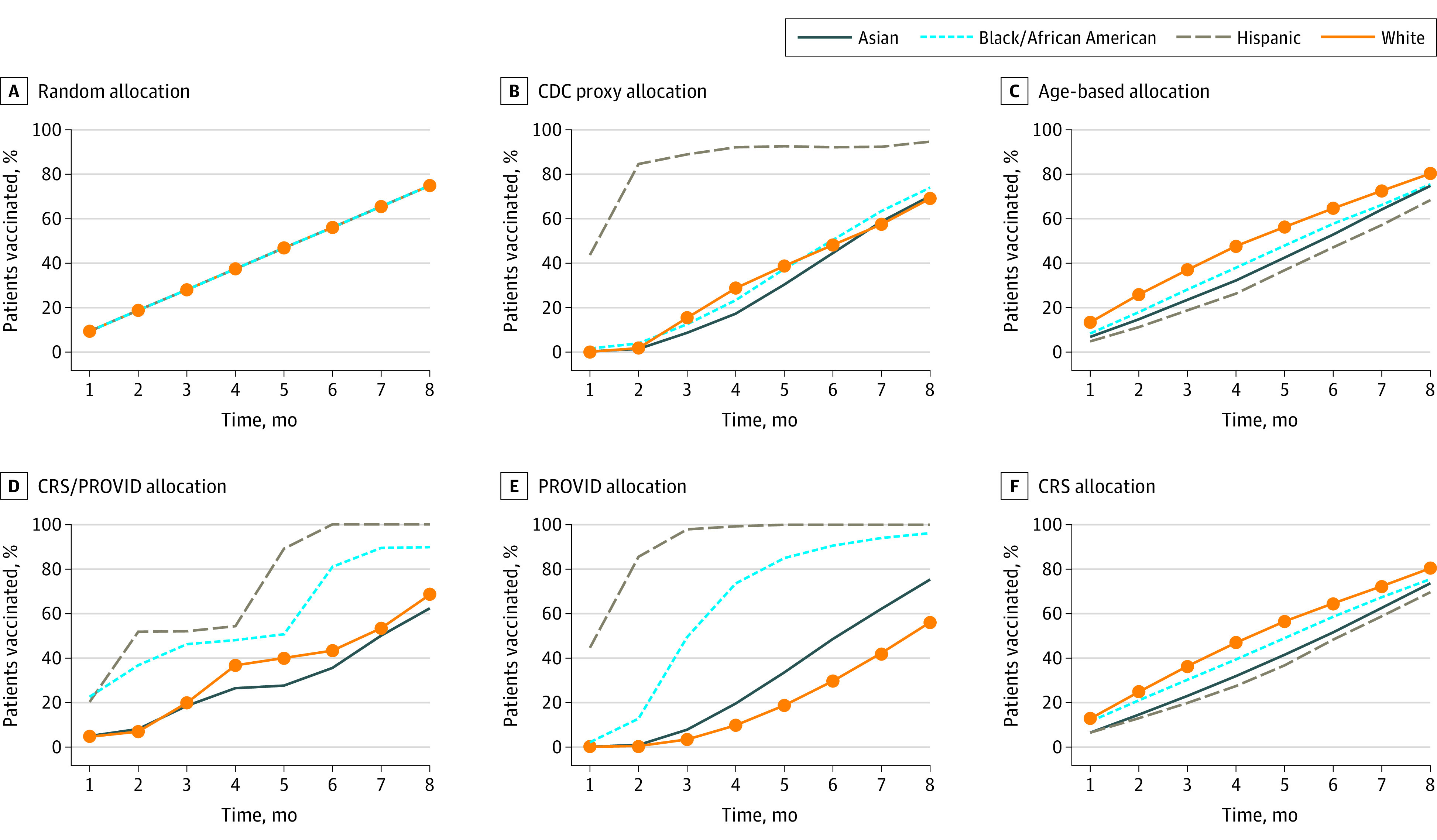
We simulated the association of different vaccine allocation strategies, including (1) random, (2) a US Centers for Disease Control and Prevention (CDC) proxy, (3) age based, and (4) combinations of models for the risk of adverse outcomes (CRS) and COVID-19 infection (PROVID), with COVID-19-related hospitalizations between May 1, 2020, and December 31, 2020, that were randomly permuted by month across 250 simulations and assessed vaccine allocation by race and ethnicity and the neighborhood deprivation index across time.
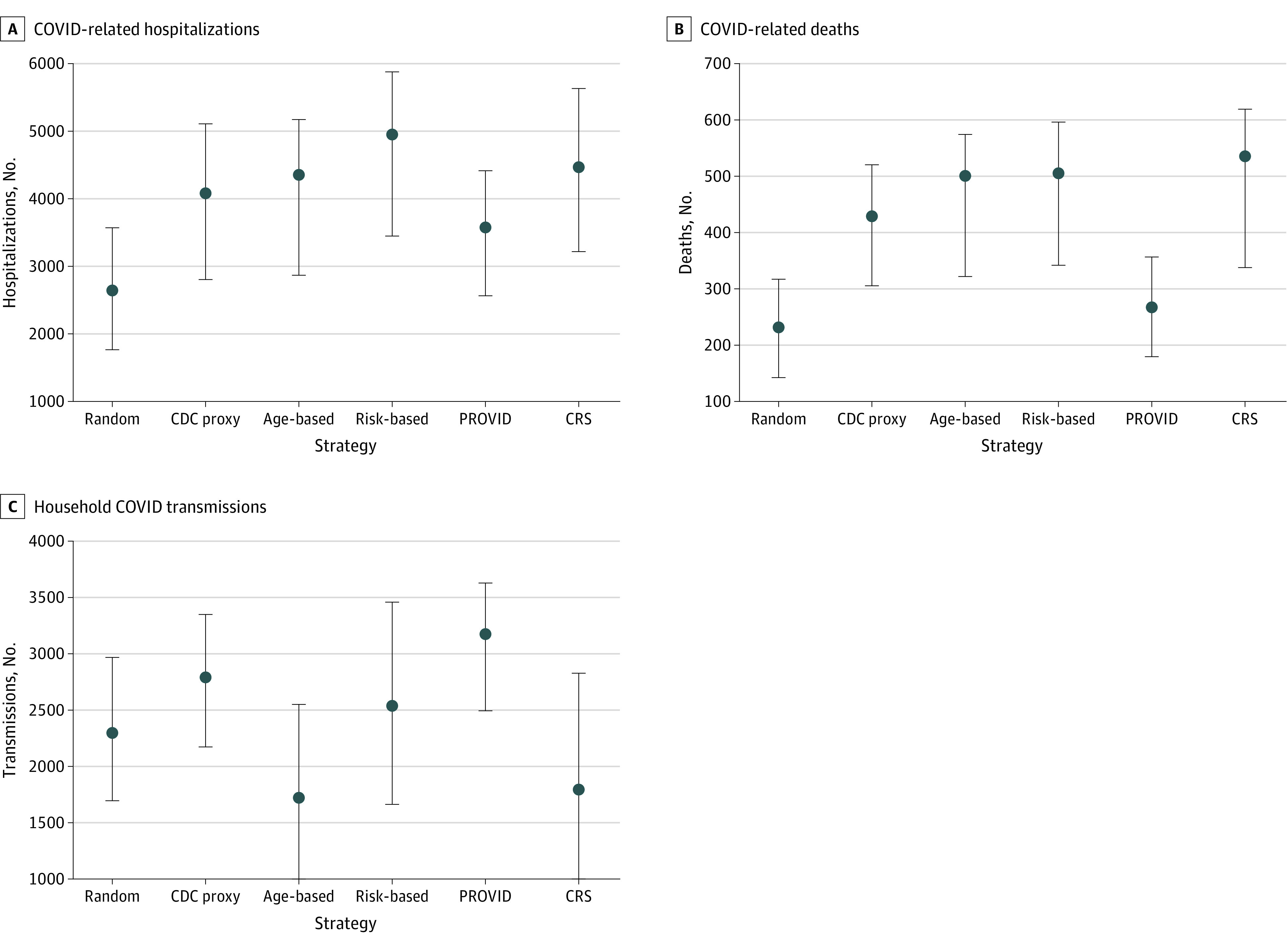
The study included 3 202 679 adult patients (mean [SD] age, 48.2 [18.0] years; 1 677 637 women [52.4%]; 1 525 042 men [47.6%]; 611 154 Asian [19.1%], 206 363 Black [6.4%], 642 344 Hispanic [20.1%], and 1 390 638 White individuals [43.4%]), of whom 36 137 (1.1%) were positive for SARS-CoV-2. A risk-based strategy (CRS/PROVID) showed the largest avoidable hospitalization estimates (4954; 95% CI, 3452-5878) followed by age-based (4362; 95% CI, 2866-5175) and CDC proxy (4085; 95% CI, 2805-5109) strategies. Random vaccination showed substantially lower reductions in adverse outcomes. Risk-based strategies also showed the largest number of avoidable COVID-19 deaths (joint CRS/PROVID) and household transmissions. Risk-based (PROVID) and CDC proxy strategies were estimated to vaccinate the highest percentage of Hispanic and Black patients in 8 months (joint CRS/PROVID: 642 570 [100%] Hispanic, 185 530 [90%] Black; PROVID: 642 570 [100%] Hispanic, 198 480 [96%] Black; CDC proxy: 605 770 [95%] Hispanic and 151 772 [74%] Black) compared with an age-based approach (438 423 [68%] Hispanic, 154 714 [75%] Black). Overall, the PROVID and joint CRS/PROVID risk-based strategies were estimated to be followed by the most patients from areas with high neighborhood deprivation index being vaccinated early.
In this simulation modeling study of adults from a large integrated health care delivery system, risk-based strategies were associated with the largest estimated reductions in COVID-19 hospitalizations, deaths, and household transmissions compared with the CDC proxy and age-based strategies, with a higher proportion of Hispanic and Black patients were estimated to be vaccinated early in the process compared with the CDC strategy.
确定最有效的 COVID-19 疫苗分配策略可能会显著减少住院人数并挽救生命,同时确保公平分配疫苗。
模拟不同疫苗分配策略与 COVID-19 相关发病率和死亡率的关联及其在种族和族裔群体中的分布。
设计、设置和参与者:我们在随机分割的训练和验证数据集上开发并内部验证了 COVID-19 感染风险和住院风险模型。这些模型用于对来自综合医疗服务提供系统的成年健康计划成员进行疫苗优先排序的计算机模拟研究。该研究于 2021 年 1 月 3 日至 6 月 1 日在加利福尼亚州奥克兰进行,同期进行数据分析。
我们模拟了不同疫苗分配策略(1)随机、(2)美国疾病控制与预防中心(CDC)代理、(3)基于年龄和(4)风险不良结果(CRS)和 COVID-19 感染(PROVID)模型的组合)与 2020 年 5 月 1 日至 2020 年 12 月 31 日期间 COVID-19 相关住院之间的关联,这些关联在 250 次随机模拟中通过月份随机排列,并按种族和族裔以及时间评估疫苗分配情况。
该研究包括 3202679 名成年患者(平均[标准差]年龄 48.2[18.0]岁;1677637 名女性[52.4%];1525042 名男性[47.6%];611154 名亚裔[19.1%],206363 名黑人[6.4%],642344 名西班牙裔[20.1%]和 1390638 名白人个体[43.4%]),其中 36137(1.1%)人 SARS-CoV-2 检测呈阳性。基于风险的策略(CRS/PROVID)显示最大的可避免住院估计数(4954;95%CI,3452-5878),其次是基于年龄的策略(4362;95%CI,2866-5175)和 CDC 代理策略(4085;95%CI,2805-5109)。随机接种疫苗可显著降低不良结果的发生。基于风险的策略还显示出最大数量的可避免 COVID-19 死亡(联合 CRS/PROVID)和家庭传播。基于风险的(PROVID)和 CDC 代理策略估计在 8 个月内为最高比例的西班牙裔和黑人患者接种疫苗(联合 CRS/PROVID:642570[100%]西班牙裔,185530[90%]黑人;PROVID:642570[100%]西班牙裔,198480[96%]黑人;CDC 代理:605770[95%]西班牙裔和 151772[74%]黑人),而不是基于年龄的方法(438423[68%]西班牙裔,154714[75%]黑人)。总体而言,与 CDC 代理和基于年龄的策略相比,基于风险的策略预计将使更多来自高社区剥夺指数地区的患者早期接种疫苗。
在这项针对来自大型综合医疗服务提供系统的成年人的模拟建模研究中,与 CDC 代理和基于年龄的策略相比,基于风险的策略与 COVID-19 住院、死亡和家庭传播的最大估计减少相关,与 CDC 策略相比,预计更多的西班牙裔和黑人患者将在早期阶段接种疫苗。