Precision Monitoring to Transform Care Quality Enhancement Research Initiative, Health Services Research and Development, Department of Veterans Affairs, Indianapolis, Indiana.
Health Services Research and Development Center for Health Information and Communication, Richard L. Roudebush VA Medical Center, Department of Veterans Affairs, Indianapolis, Indiana.
JAMA Netw Open. 2021 Jan 4;4(1):e2034266. doi: 10.1001/jamanetworkopen.2020.34266.
Although strain on hospital capacity has been associated with increased mortality in nonpandemic settings, studies are needed to examine the association between coronavirus disease 2019 (COVID-19) critical care capacity and mortality.
To examine whether COVID-19 mortality was associated with COVID-19 intensive care unit (ICU) strain.
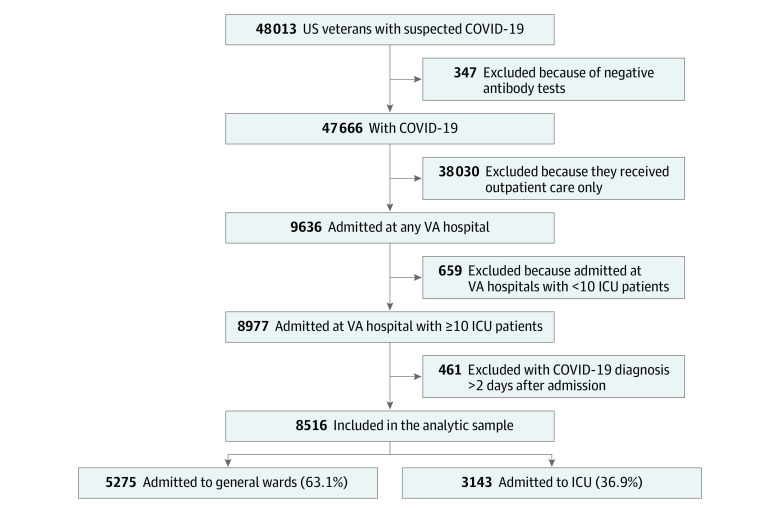
DESIGN, SETTING, AND PARTICIPANTS: This cohort study was conducted among veterans with COVID-19, as confirmed by polymerase chain reaction or antigen testing in the laboratory from March through August 2020, cared for at any Department of Veterans Affairs (VA) hospital with 10 or more patients with COVID-19 in the ICU. The follow-up period was through November 2020. Data were analyzed from March to November 2020.
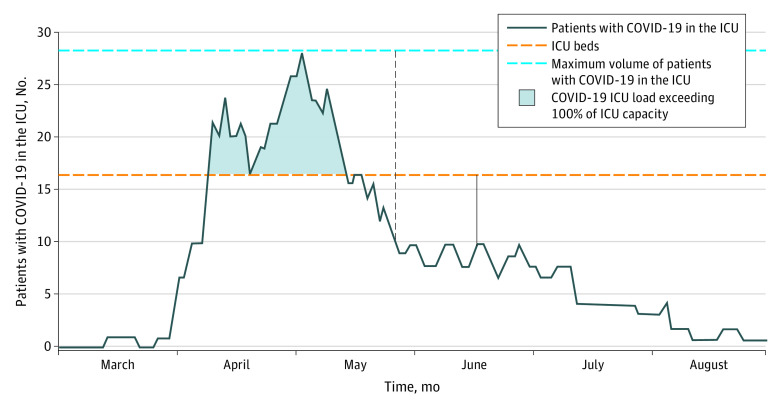
Receiving treatment for COVID-19 in the ICU during a period of increased COVID-19 ICU load, with load defined as mean number of patients with COVID-19 in the ICU during the patient's hospital stay divided by the number of ICU beds at that facility, or increased COVID-19 ICU demand, with demand defined as mean number of patients with COVID-19 in the ICU during the patient's stay divided by the maximum number of patients with COVID-19 in the ICU.
All-cause mortality was recorded through 30 days after discharge from the hospital.
Among 8516 patients with COVID-19 admitted to 88 VA hospitals, 8014 (94.1%) were men and mean (SD) age was 67.9 (14.2) years. Mortality varied over time, with 218 of 954 patients (22.9%) dying in March, 399 of 1594 patients (25.0%) dying in April, 143 of 920 patients (15.5%) dying in May, 179 of 1314 patients (13.6%) dying in June, 297 of 2373 patients (12.5%) dying in July, and 174 of 1361 (12.8%) patients dying in August (P < .001). Patients with COVID-19 who were treated in the ICU during periods of increased COVID-19 ICU demand had increased risk of mortality compared with patients treated during periods of low COVID-19 ICU demand (ie, demand of ≤25%); the adjusted hazard ratio for all-cause mortality was 0.99 (95% CI, 0.81-1.22; P = .93) for patients treated when COVID-19 ICU demand was more than 25% to 50%, 1.19 (95% CI, 0.95-1.48; P = .13) when COVID-19 ICU demand was more than 50% to 75%, and 1.94 (95% CI, 1.46-2.59; P < .001) when COVID-19 ICU demand was more than 75% to 100%. No association between COVID-19 ICU demand and mortality was observed for patients with COVID-19 not in the ICU. The association between COVID-19 ICU load and mortality was not consistent over time (ie, early vs late in the pandemic).
This cohort study found that although facilities augmented ICU capacity during the pandemic, strains on critical care capacity were associated with increased COVID-19 ICU mortality. Tracking COVID-19 ICU demand may be useful to hospital administrators and health officials as they coordinate COVID-19 admissions across hospitals to optimize outcomes for patients with this illness.
尽管医院容量的压力与非大流行环境下的死亡率增加有关,但仍需要研究 2019 年冠状病毒病(COVID-19)重症监护能力与死亡率之间的关系。
研究 COVID-19 重症监护室(ICU)压力与 COVID-19 死亡率之间是否存在关联。
设计、地点和参与者:这项队列研究在退伍军人中进行,这些退伍军人通过实验室聚合酶链反应或抗原检测确诊为 COVID-19,在 2020 年 3 月至 8 月期间在任何拥有 10 名或以上 COVID-19 ICU 患者的退伍军人事务部(VA)医院接受治疗。随访期截止到 2020 年 11 月。数据分析于 2020 年 3 月至 11 月进行。
在 COVID-19 ICU 负荷增加期间(定义为患者住院期间 COVID-19 ICU 患者的平均人数除以该设施的 ICU 床位数)或 COVID-19 ICU 需求增加期间(定义为患者住院期间 COVID-19 ICU 患者的平均人数除以 COVID-19 ICU 患者的最大人数)接受 COVID-19 ICU 治疗。
通过出院后 30 天记录全因死亡率。
在 88 家 VA 医院收治的 8516 名 COVID-19 患者中,8014 名(94.1%)为男性,平均(SD)年龄为 67.9(14.2)岁。死亡率随时间而变化,3 月有 954 名患者中的 218 名(22.9%)死亡,4 月有 1594 名患者中的 399 名(25.0%)死亡,5 月有 920 名患者中的 143 名(15.5%)死亡,6 月有 1314 名患者中的 179 名(13.6%)死亡,7 月有 2373 名患者中的 297 名(12.5%)死亡,8 月有 1361 名患者中的 174 名(12.8%)死亡(P<0.001)。与 COVID-19 低 ICU 需求期间(即需求≤25%)相比,在 COVID-19 ICU 需求增加期间接受 ICU 治疗的 COVID-19 患者死亡风险增加,所有原因死亡率的调整后危害比为 0.99(95%CI,0.81-1.22;P=0.93),COVID-19 ICU 需求超过 25%至 50%时为 1.19(95%CI,0.95-1.48;P=0.13),COVID-19 ICU 需求超过 50%至 75%时为 1.48(95%CI,0.95-1.48;P=0.13),COVID-19 ICU 需求超过 75%至 100%时为 1.94(95%CI,1.46-2.59;P<0.001)。在没有入住 ICU 的 COVID-19 患者中,COVID-19 ICU 需求与死亡率之间没有关联。COVID-19 ICU 负荷与死亡率之间的关系在整个疫情期间并不一致(即早期与晚期)。
这项队列研究发现,尽管在大流行期间医院增加了 ICU 容量,但 ICU 压力与 COVID-19 ICU 死亡率增加有关。跟踪 COVID-19 ICU 需求可能对医院管理人员和卫生官员有用,因为他们协调医院的 COVID-19 入院,以优化患有这种疾病的患者的结果。