Huo Ben-Nian, Wu Yue-E, Shu Ling, Zhang Ruo-Qi, Xiao Jian-Wen, Li Qian-Bo, Zhao Wei, Jia Yun-Tao, Song Lin
Ministry of Education Key Laboratory of Child Development and Disorders, Chongqing Key Laboratory of Pediatrics, Department of Pharmacy, National Clinical Research Center for Child Health and Disorders, Children's Hospital of Chongqing Medical University, Chongqing, China.
Key Laboratory of Chemical Biology (Ministry of Education), Department of Clinical Pharmacy, School of Pharmaceutical Sciences, Cheeloo College of Medicine, Shandong University, Jinan, China.
Front Pharmacol. 2022 Aug 1;13:926711. doi: 10.3389/fphar.2022.926711. eCollection 2022.
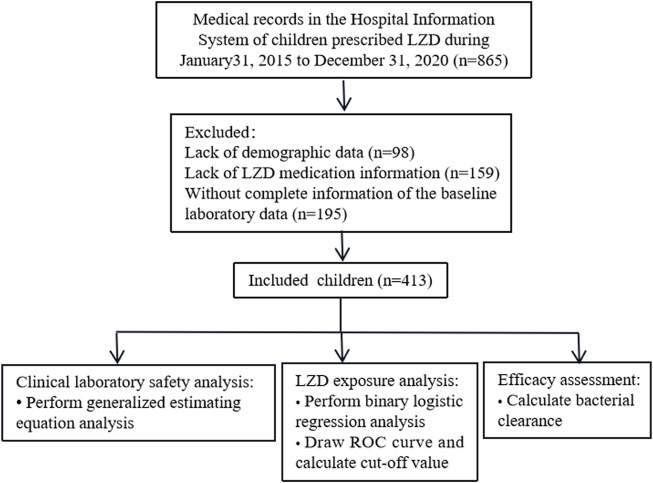
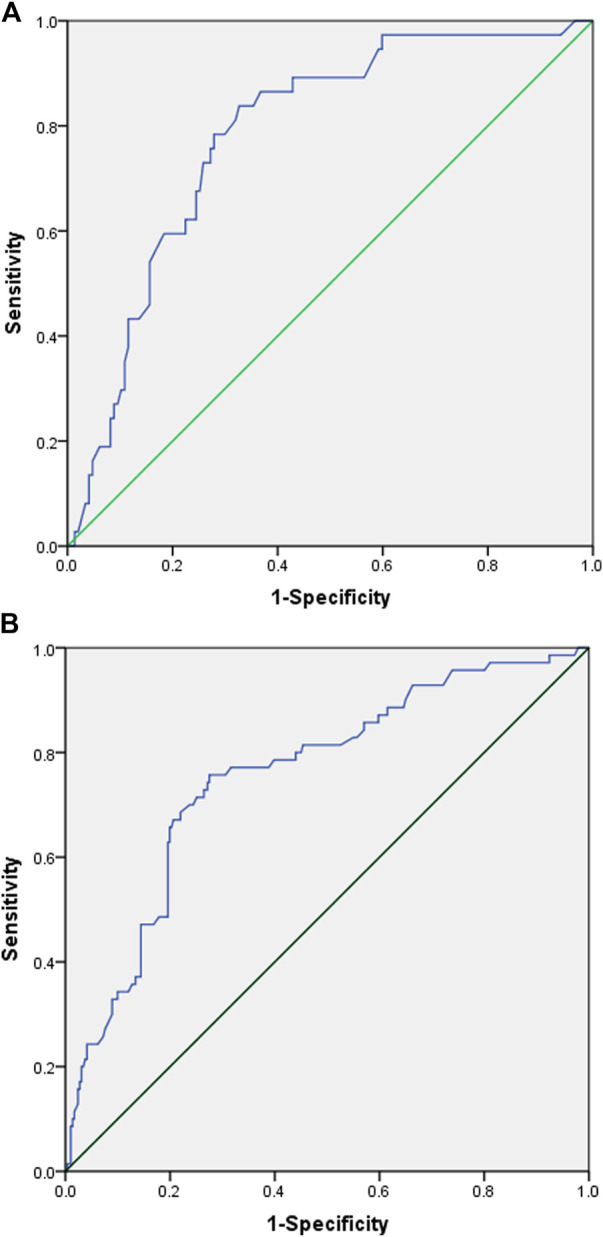
There have been limited studies concerning the safety and efficacy of linezolid (LZD) in children. This study aimed to evaluate the association between LZD exposure and clinical safety and efficacy in Chinese pediatric patients. This retrospective cross-sectional study included patients ≤18 years of age who received ≥3 days of LZD treatment between 31 January 2015, and 31 December 2020. Demographic characteristics, medication information, laboratory test information, and bacterial culture results were collected from the Hospital Information System (HIS). Exposure was defined as AUC and calculated by the non-linear mixed-effects modeling program (NONMEM), version 7.2, based on two validated population pharmacokinetic models. Binary logistic regression analyses were performed to analyze the associations between AUC and laboratory adverse events, and receiver operating characteristic curves were used to calculate the cut-off values. Efficacy was evaluated by bacterial clearance. A total of 413 paediatric patients were included, with an LZD median (interquartile range) dose, duration, clearance and AUC of 30.0 (28.1-31.6) mg/kg/day, 8 (4‒15) days,1.31 (1.29-1.32) L/h and 81.1 (60.6-108.7) mg/L·h, respectively. Adverse events associated with TBil, AST, ALT, PLT, hemoglobin, WBC, and neutrophil count increased during and after LZD treatment when compared with before medication ( < 0.05), and the most common adverse events were thrombocytopaenia (71/399, 17.8%) and low hemoglobin (61/401, 15.2%) during the LZD treatment. Patients with AUC higher than 120.69 mg/L h might be associated with low hemoglobin 1-7 days after the end of the LZD treatment, and those with an AUC higher than 92.88 mg/L∙h might be associated with thrombocytopaenia 8-15 days after the end of the LZD treatment. A total of 136 patients underwent bacterial culture both before and after LZD treatment, and the infection was cleared in 92.6% (126/136) of the patients, of whom 69.8% (88/126) had AUC/MIC values greater than 80. Hematological indicators should be carefully monitored during LZD treatment, especially thrombocytopaenia and low hemoglobin, and a continuous period of monitoring after LZD withdrawal is also necessary. Since the AUC cut-off values for laboratory adverse events were relatively low, a trade-off is necessary between the level of drug exposure required for treatment and safety, and the exposure target (AUC/MIC) in pediatric patients should be further studied, especially for patients with complications and concomitant medications.
关于利奈唑胺(LZD)在儿童中的安全性和有效性的研究有限。本研究旨在评估中国儿科患者中LZD暴露与临床安全性和有效性之间的关联。这项回顾性横断面研究纳入了2015年1月31日至2020年12月31日期间接受LZD治疗≥3天的18岁及以下患者。从医院信息系统(HIS)收集人口统计学特征、用药信息、实验室检查信息和细菌培养结果。暴露定义为AUC,并基于两个经过验证的群体药代动力学模型,由非线性混合效应建模程序(NONMEM)7.2版计算得出。进行二元逻辑回归分析以分析AUC与实验室不良事件之间的关联,并使用受试者工作特征曲线计算临界值。通过细菌清除率评估疗效。共纳入413例儿科患者,LZD的中位(四分位间距)剂量、疗程、清除率和AUC分别为30.0(28.1 - 31.6)mg/kg/天、8(4 - 15)天、1.31(1.29 - 1.32)L/h和81.1(60.6 - 108.7)mg/L·h。与用药前相比,LZD治疗期间及治疗后与总胆红素、谷草转氨酶、谷丙转氨酶、血小板、血红蛋白、白细胞和中性粒细胞计数相关的不良事件增加(P < 0.05),LZD治疗期间最常见的不良事件是血小板减少症(71/399,17.8%)和低血红蛋白(61/401,15.2%)。LZD治疗结束后1 - 7天,AUC高于120.69 mg/L h的患者可能与低血红蛋白有关,而LZD治疗结束后8 - 15天,AUC高于92.88 mg/L∙h的患者可能与血小板减少症有关。共有136例患者在LZD治疗前后均进行了细菌培养,92.6%(126/136)的患者感染得到清除,其中69.8%(88/126)的患者AUC/MIC值大于80。LZD治疗期间应仔细监测血液学指标,尤其是血小板减少症和低血红蛋白,LZD停药后也需要持续监测一段时间。由于实验室不良事件的AUC临界值相对较低,治疗所需的药物暴露水平与安全性之间需要进行权衡,儿科患者的暴露目标(AUC/MIC)应进一步研究,尤其是对于有并发症和合并用药的患者。