Gastroenterological Surgery, Helsinki University Hospital and University of Helsinki, Helsinki, Finland.
Division of Surgery, Department of Clinical Science, Intervention, and Technology, Karolinska Institutet, Stockholm, Sweden.
Br J Surg. 2022 Oct 14;109(11):1131-1139. doi: 10.1093/bjs/znac266.
Highly utilized risk scores for clinically relevant postoperative pancreatic fistula (CR-POPF) have guided clinical decision-making in pancreatoduodenectomy. However, none has been successfully developed for distal pancreatectomy. This study aimed to develop and validate a new fistula risk score for distal pancreatectomy.
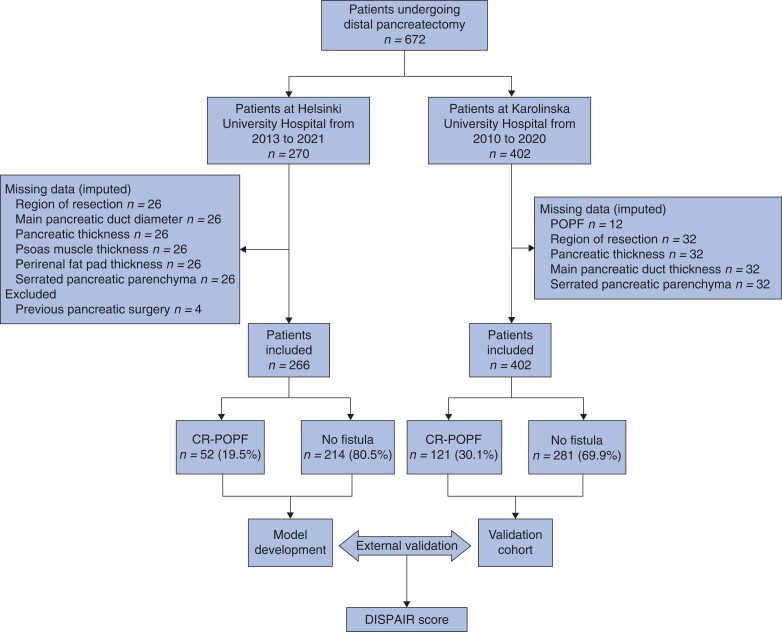
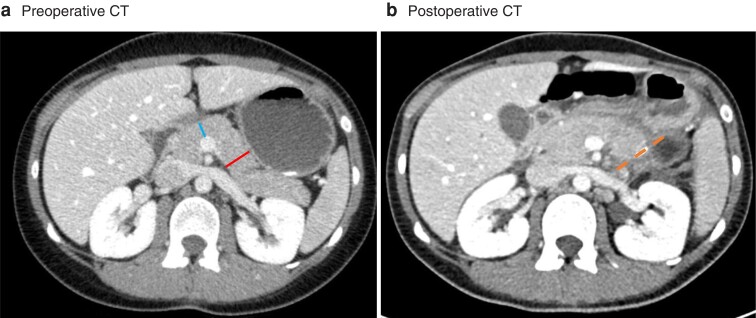
Patients undergoing distal pancreatectomy at Helsinki University Hospital, Finland from 2013 to 2021, and at Karolinska University Hospital, Sweden, from 2010 to 2020, were included retrospectively. The outcome was CR-POPF, according to the 2016 International Study Group of Pancreatic Surgery definition. Preoperative clinical demographics and radiological parameters such as pancreatic thickness and duct diameter were measured. A logistic regression model was developed, internally validated with bootstrapping, and the performance assessed in an external validation cohort.
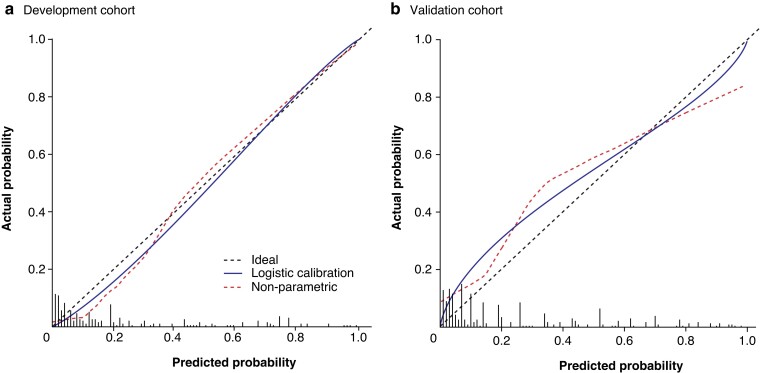
Of 668 patients from Helsinki (266) and Stockholm (402), 173 (25.9 per cent) developed CR-POPF. The final model consisted of three variables assessed before surgery: transection site (neck versus body/tail), pancreatic thickness at transection site, and diabetes. The model had an area under the receiver operating characteristic curve (AUROC) of 0.904 (95 per cent c.i. 0.855 to 0.949) after internal validation, and 0.798 (0.748 to 0.848) after external validation. The calibration slope and intercept on external validation were 0.719 and 0.192 respectively. Four risk groups were defined in the validation cohort for clinical applicability: low (below 5 per cent), moderate (at least 5 but below 30 per cent), high (at least 30 but below 75 per cent), and extreme (75 per cent or more). The incidences in these groups were 8.7 per cent (11 of 126), 22.0 per cent (36 of 164), 63 per cent (57 of 91), and 81 per cent (17 of 21) respectively.
The DISPAIR score after distal pancreatectomy may guide decision-making and allow a risk-adjusted outcome comparison for CR-POPF.
临床上相关的术后胰瘘(CR-POPF)的高度利用风险评分指导了胰十二指肠切除术的临床决策。然而,对于胰体尾切除术,尚未成功开发出此类评分。本研究旨在开发和验证胰体尾切除术新的瘘管风险评分。
回顾性纳入 2013 年至 2021 年在芬兰赫尔辛基大学医院和 2010 年至 2020 年在瑞典卡罗林斯卡大学医院接受胰体尾切除术的患者。根据 2016 年国际胰腺外科学研究组的定义,将结果定义为 CR-POPF。测量术前临床人口统计学和影像学参数,如胰腺厚度和胰管直径。建立逻辑回归模型,通过自举法进行内部验证,并在外部验证队列中评估其性能。
在来自赫尔辛基(266 例)和斯德哥尔摩(402 例)的 668 例患者中,有 173 例(25.9%)发生了 CR-POPF。最终模型包含三个术前评估的变量:切断部位(颈部与体尾部/尾部)、切断部位的胰腺厚度和糖尿病。该模型的内部验证的受试者工作特征曲线下面积(AUROC)为 0.904(95%置信区间 0.855 至 0.949),外部验证的 AUROC 为 0.798(0.748 至 0.848)。外部验证的校准斜率和截距分别为 0.719 和 0.192。为了便于临床应用,在验证队列中定义了四个风险组:低(<5%)、中(至少 5%但<30%)、高(至少 30%但<75%)和极高(75%或更高)。这些组的发生率分别为 8.7%(11/126)、22.0%(36/164)、63.0%(57/91)和 81.0%(17/21)。
胰体尾切除术后的 DISPAIR 评分可以指导决策,并允许对 CR-POPF 进行风险调整后的结果比较。