Clinical Trials and Statistics Unit (ICR-CTSU)- Division of Clinical Studies, The Institute of Cancer Research, London, UK.
Royal Marsden Hospital, London, UK; The Breast Cancer Now Toby Robins Research Centre, The Institute of Cancer Research, London, UK.
EBioMedicine. 2022 Sep;83:104205. doi: 10.1016/j.ebiom.2022.104205. Epub 2022 Aug 16.
Oestrogen receptor positive/ human epidermal growth factor receptor positive (ER+/HER2+) breast cancers (BCs) are less responsive to endocrine therapy than ER+/HER2- tumours. Mechanisms underpinning the differential behaviour of ER+HER2+ tumours are poorly characterised. Our aim was to identify biomarkers of response to 2 weeks' presurgical AI treatment in ER+/HER2+ BCs.
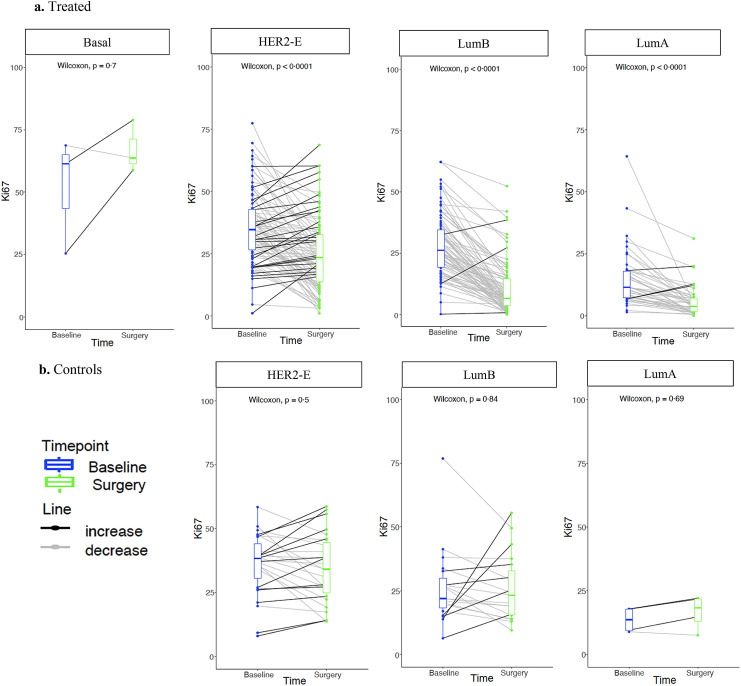
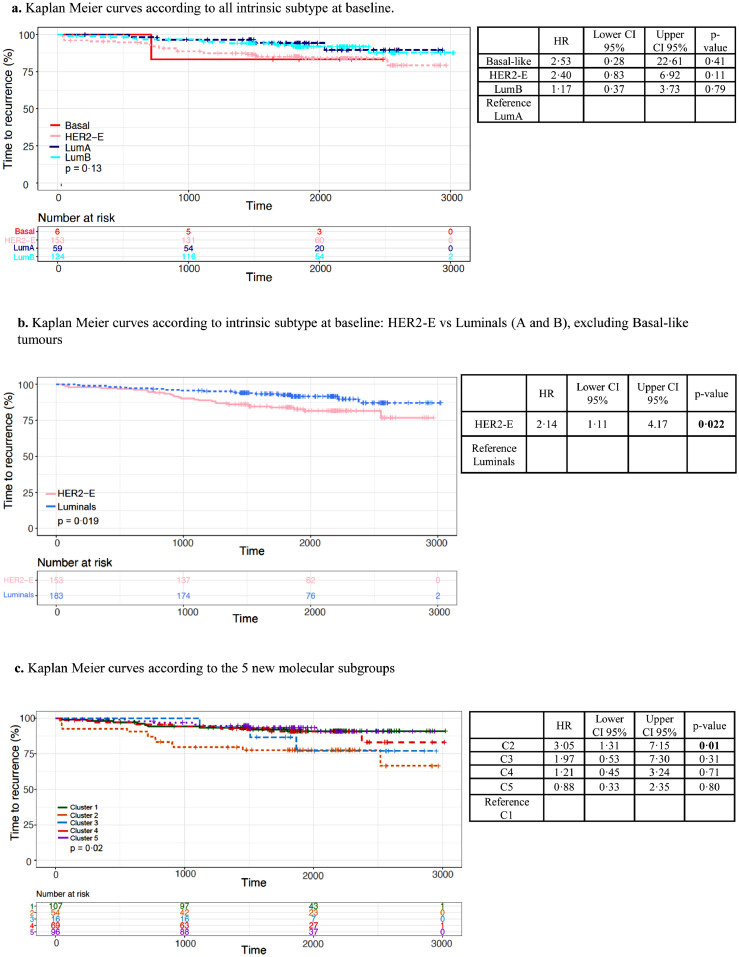
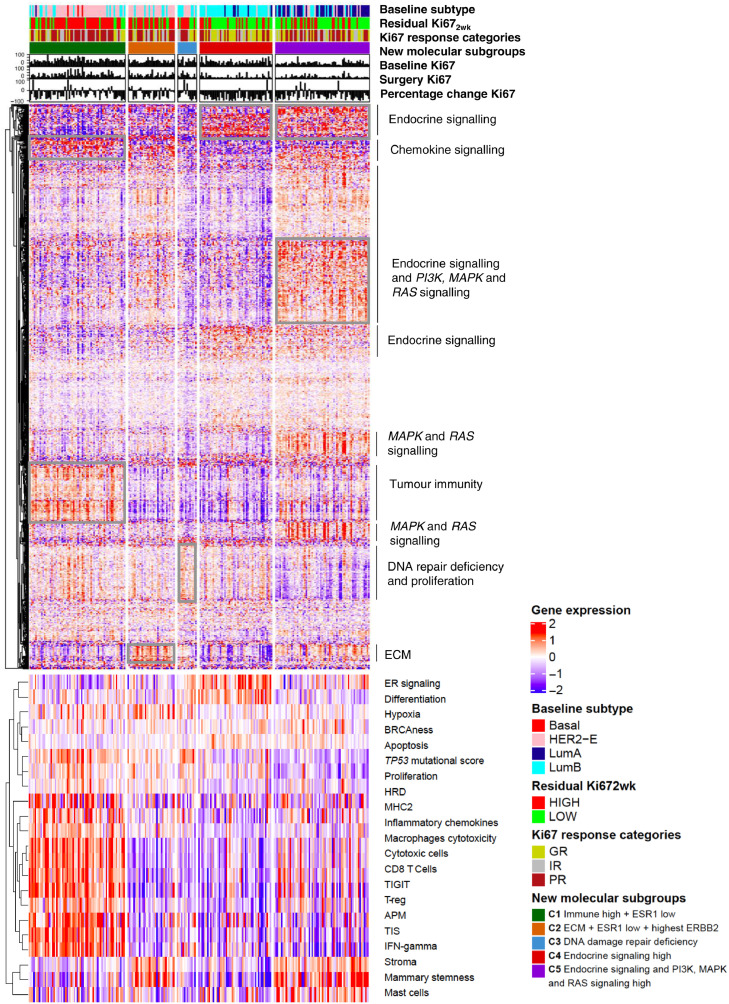
All available ER+/HER2+ BC baseline tumours (n=342) in the POETIC trial were gene expression profiled using BC360™ (NanoString) covering intrinsic subtypes and 46 key biological signatures. Early response to AI was assessed by changes in Ki67 expression and residual Ki67 at 2 weeks (Ki67). Time-To-Recurrence (TTR) was estimated using Kaplan-Meier methods and Cox models adjusted for standard clinicopathological variables. New molecular subgroups (MS) were identified using consensus clustering.
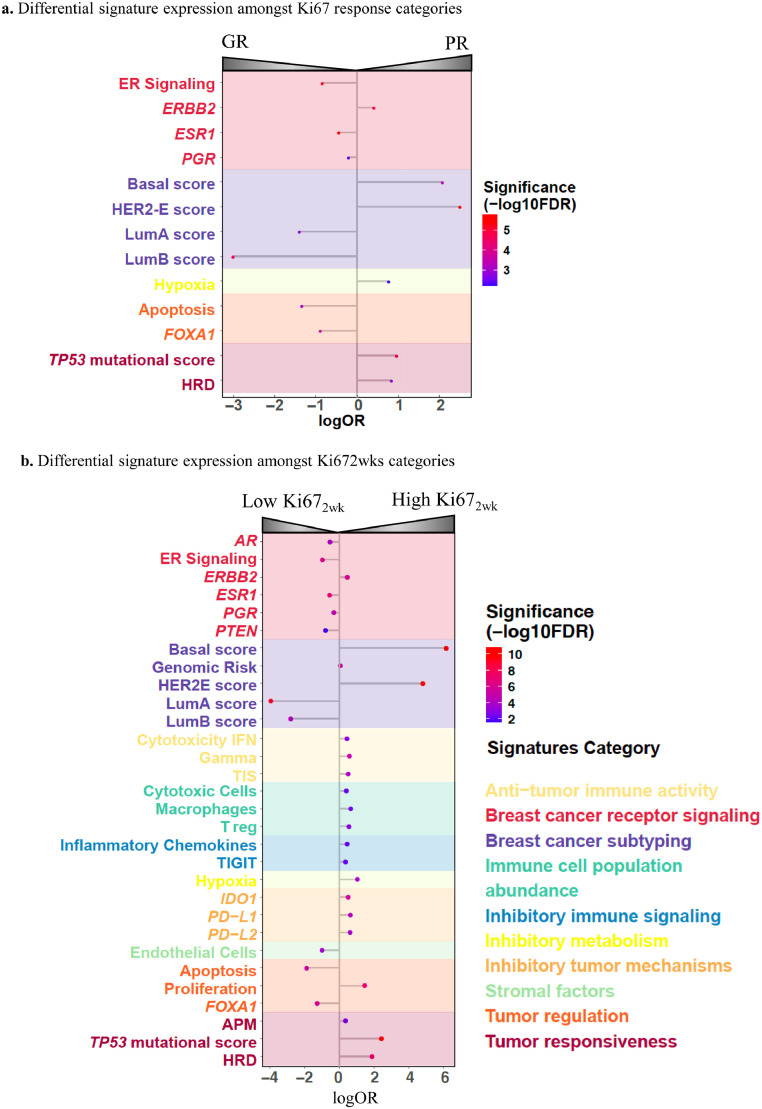
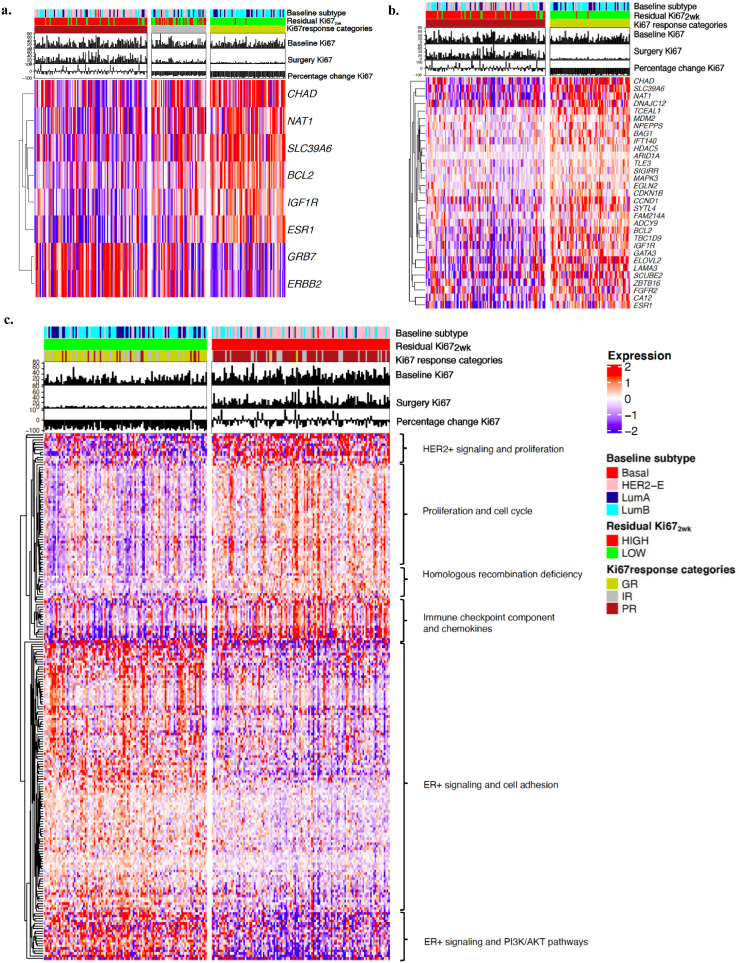
HER2-enriched (HER2-E) subtype BCs (44.7% of the total) showed poorer Ki67 response and higher Ki67 (p<0.0001) than non-HER2-E BCs. High expression of ERBB2 expression, homologous recombination deficiency (HRD) and TP53 mutational score were associated with poor response and immune-related signatures with High Ki67. Five new MS that were associated with differential response to AI were identified. HER2-E had significantly poorer TTR compared to Luminal BCs (HR 2.55, 95% CI 1.14-5.69; p=0.0222). The new MS were independent predictors of TTR, adding significant value beyond intrinsic subtypes.
Our results show HER2-E as a standardised biomarker associated with poor response to AI and worse outcome in ER+/HER2+. HRD, TP53 mutational score and immune-tumour tolerance are predictive biomarkers for poor response to AI. Lastly, novel MS identify additional non-HER2-E tumours not responding to AI with an increased risk of relapse.
Cancer Research UK (CRUK/07/015).
雌激素受体阳性/人表皮生长因子受体阳性(ER+/HER2+)乳腺癌(BC)对内分泌治疗的反应不如 ER+/HER2-肿瘤敏感。ER+HER2+肿瘤表现出不同行为的机制尚未得到充分描述。我们的目的是确定 ER+/HER2+BC 接受 2 周术前 AI 治疗的反应生物标志物。
POETIC 试验中所有可用的 ER+/HER2+BC 基线肿瘤(n=342)均使用 BC360™(NanoString)进行基因表达谱分析,涵盖了内在亚型和 46 个关键生物学特征。通过 Ki67 表达的变化和 2 周时的残留 Ki67(Ki67)来评估 AI 的早期反应。使用 Kaplan-Meier 方法和 Cox 模型估计无复发生存时间(TTR),并调整了标准临床病理变量。使用共识聚类识别新的分子亚群(MS)。
HER2 富集(HER2-E)亚型 BC(占总数的 44.7%)的 Ki67 反应较差,Ki67 更高(p<0.0001),而非 HER2-E BC 则相反。ERBB2 表达高、同源重组缺陷(HRD)和 TP53 突变评分与不良反应相关,而免疫相关特征与高 Ki67 相关。鉴定出与 AI 反应差异相关的 5 个新 MS。与 Luminal BC 相比,HER2-E 的 TTR 显著更差(HR 2.55,95%CI 1.14-5.69;p=0.0222)。新的 MS 是 TTR 的独立预测因子,除了内在亚型之外,还具有显著的附加价值。
我们的结果表明,HER2-E 是一种与 AI 反应不良和 ER+/HER2+不良预后相关的标准化生物标志物。HRD、TP53 突变评分和免疫肿瘤耐受是 AI 反应不良的预测生物标志物。最后,新的 MS 确定了另外一些对 AI 无反应的非 HER2-E 肿瘤,这些肿瘤复发风险增加。
英国癌症研究中心(CRUK/07/015)。