Division of Emergency Medicine, Ann & Robert H. Lurie Children's Hospital of Chicago, Northwestern University Feinberg School of Medicine, Chicago, Illinois.
Department of Bioinformatics and Biostatistics, University of Louisville, Louisville, Kentucky.
Hosp Pediatr. 2022 Sep 1;12(9):788-806. doi: 10.1542/hpeds.2022-006608.
To characterize the outcomes of children with community acquired pneumonia (CAP) across 41 United States hospitals and evaluate factors associated with potentially unnecessary admissions.
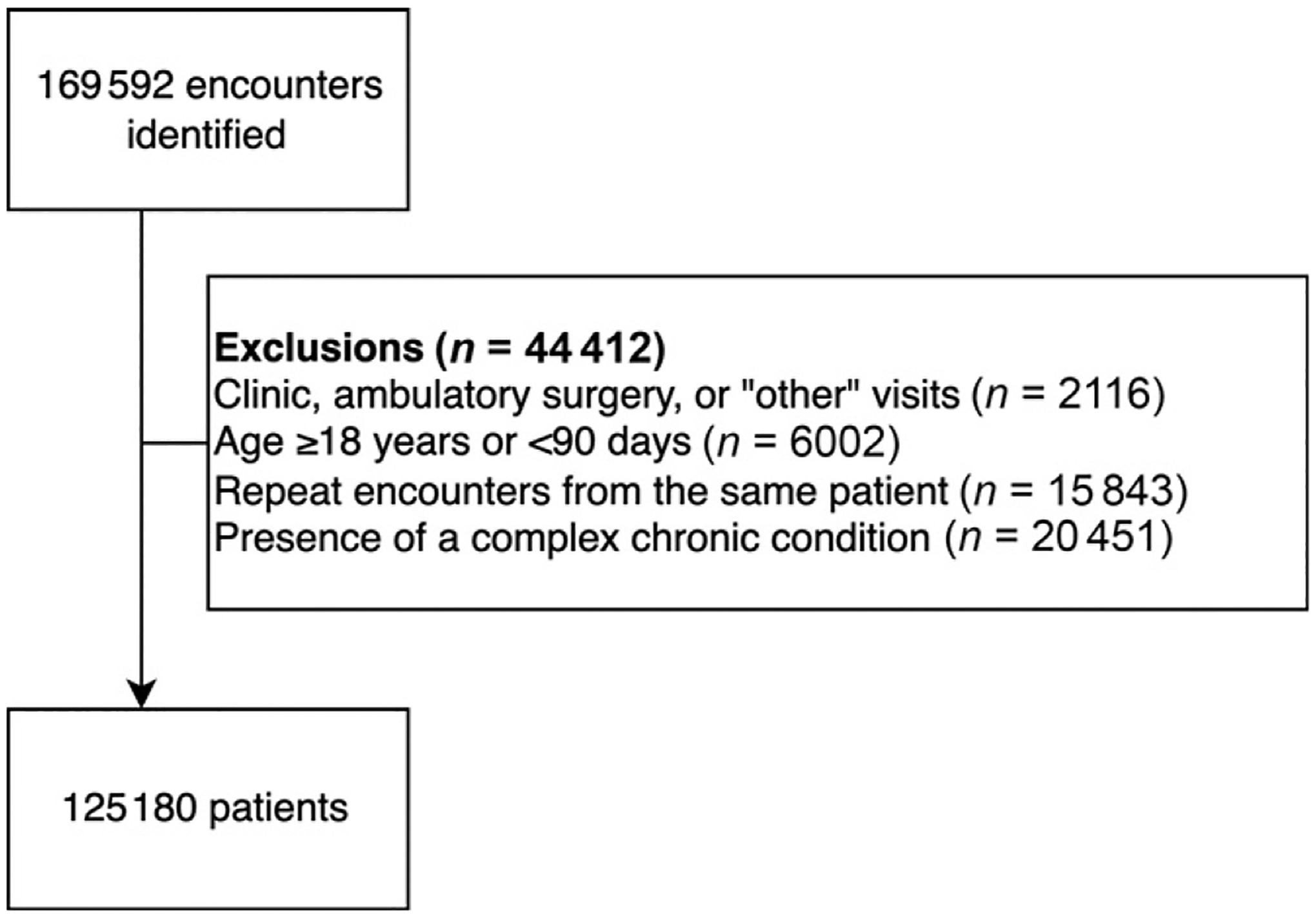
We performed a cross-sectional study of patients with CAP from 41 United States pediatric hospitals and evaluated clinical outcomes using a composite ordinal severity outcome: mild-discharged (discharged from the emergency department), mild-admitted (hospitalized without other interventions), moderate (provision of intravenous fluids, supplemental oxygen, broadening of antibiotics, complicated pneumonia, and presumed sepsis) or severe (ICU, positive-pressure ventilation, vasoactive infusion, chest drainage, extracorporeal membrane oxygenation, severe sepsis, or death). Our primary outcome was potentially unnecessary admissions (ie, mild-admitted). Among mild-discharged and mild-admitted patients, we constructed a generalized linear mixed model for mild-admitted severity and assessed the role of fixed (demographics and clinical testing) and random effects (institution) on this outcome.
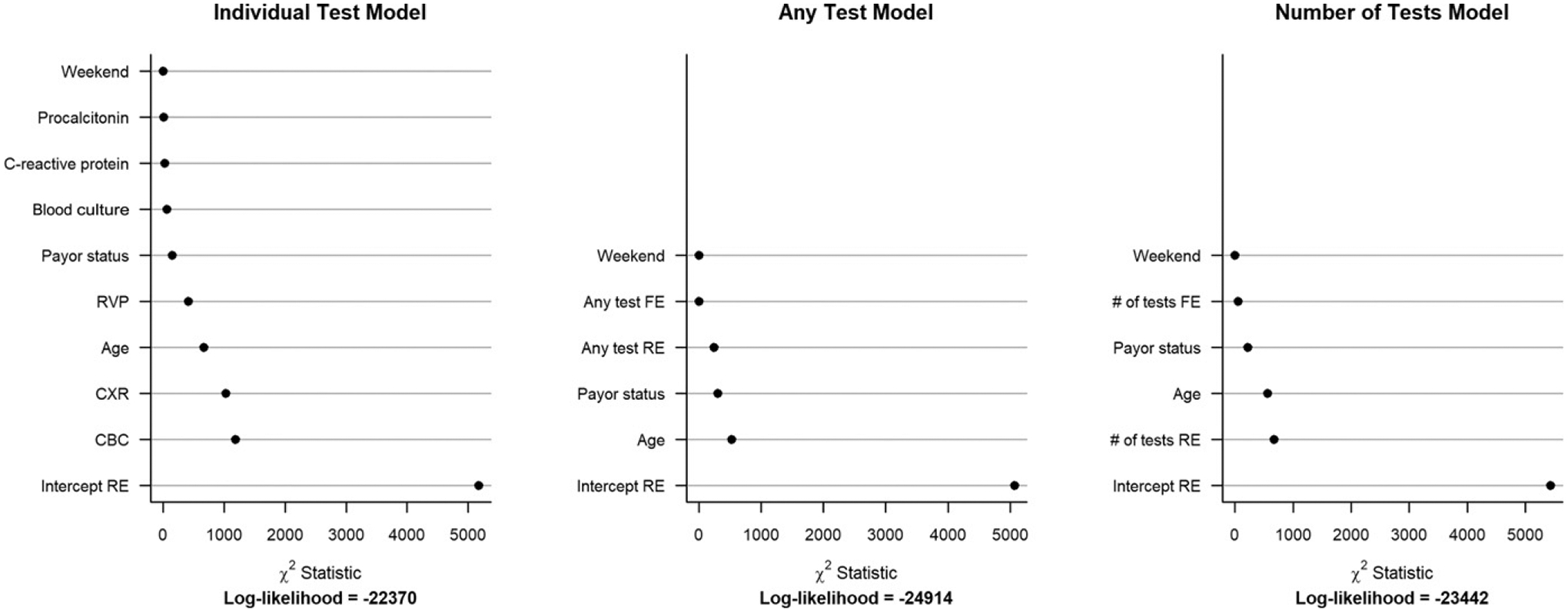
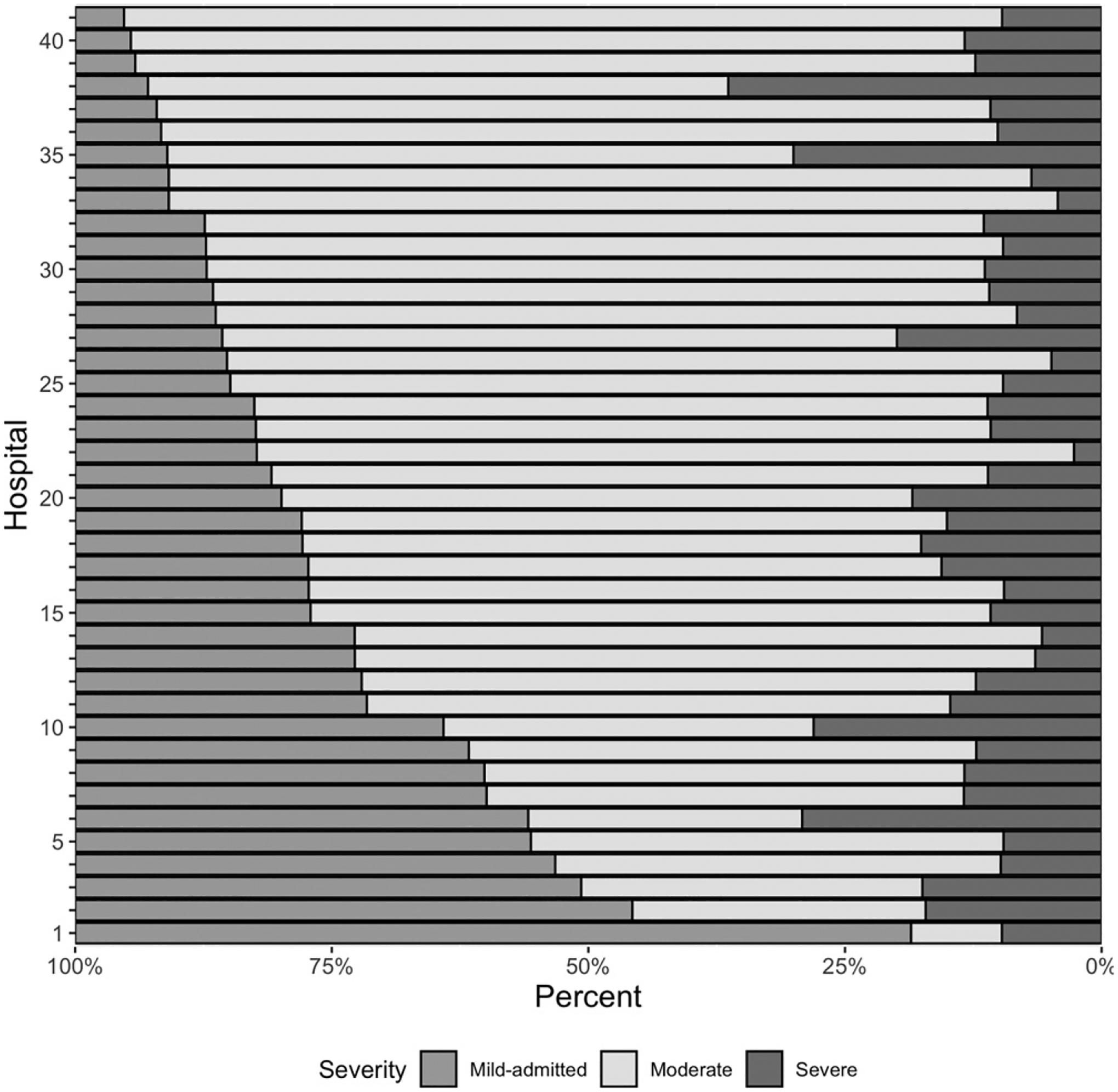
Of 125 180 children, 68.3% were classified as mild-discharged, 6.6% as mild-admitted, 20.6% as moderate and 4.5% as severe. Among admitted patients (n = 39 692), 8321 (21%) were in the mild-admitted group, with substantial variability in this group across hospitals (median 19.1%, interquartile range 12.8%-28.4%). In generalized linear mixed models comparing mild-admitted and mild-discharge severity groups, hospital had the greatest contribution to model variability compared to all other variables.
One in 5 hospitalized children with CAP do not receive significant interventions. Among patients with mild disease, institutional variation is the most important contributor to predict potentially unnecessary admissions. Improved prognostic tools are needed to reduce potentially unnecessary hospitalization of children with CAP.
描述美国 41 家医院获得性肺炎(CAP)患儿的结局,并评估与潜在不必要住院相关的因素。
我们对美国 41 家儿科医院的 CAP 患儿进行了横断面研究,使用复合有序严重程度结局评估临床结局:轻度出院(从急诊室出院)、轻度住院(无需其他干预的住院)、中度(静脉输液、补充氧气、抗生素扩大、复杂肺炎和疑似败血症)或重度(ICU、正压通气、血管活性输注、胸腔引流、体外膜氧合、严重败血症或死亡)。我们的主要结局是潜在不必要的住院(即轻度住院)。在轻度出院和轻度住院的患者中,我们构建了一个用于轻度住院严重程度的广义线性混合模型,并评估了固定(人口统计学和临床检查)和随机效应(机构)对该结果的作用。
在 125180 名儿童中,68.3%为轻度出院,6.6%为轻度住院,20.6%为中度,4.5%为重度。在住院患者(n=39692)中,8321 例(21%)为轻度住院组,各医院之间该组存在很大差异(中位数 19.1%,四分位间距 12.8%-28.4%)。在比较轻度住院和轻度出院严重程度组的广义线性混合模型中,与所有其他变量相比,医院对模型变异性的贡献最大。
每 5 名住院 CAP 患儿中就有 1 名患儿未接受重要干预。在轻度疾病患者中,机构差异是预测潜在不必要住院的最重要因素。需要改进预后工具,以减少 CAP 患儿潜在不必要的住院。