Stanford-Surgery Policy Improvement Research and Education Center (S-SPIRE), Department of Surgery, Stanford University School of Medicine, Palo Alto, CA.
Department of Surgery, Stanford University School of Medicine, Palo Alto, CA.
Ann Surg. 2023 Aug 1;278(2):e302-e308. doi: 10.1097/SLA.0000000000005691. Epub 2022 Aug 25.
The authors sought to compare the incidence of adverse cardiovascular (CV) events in older adults with primary hyperparathyroidism (PHPT) treated with parathyroidectomy versus nonoperative management.
PHPT is a common endocrine disorder that is associated with increased CV mortality, but it is not known whether parathyroidectomy reduces the incidence of adverse CV events.
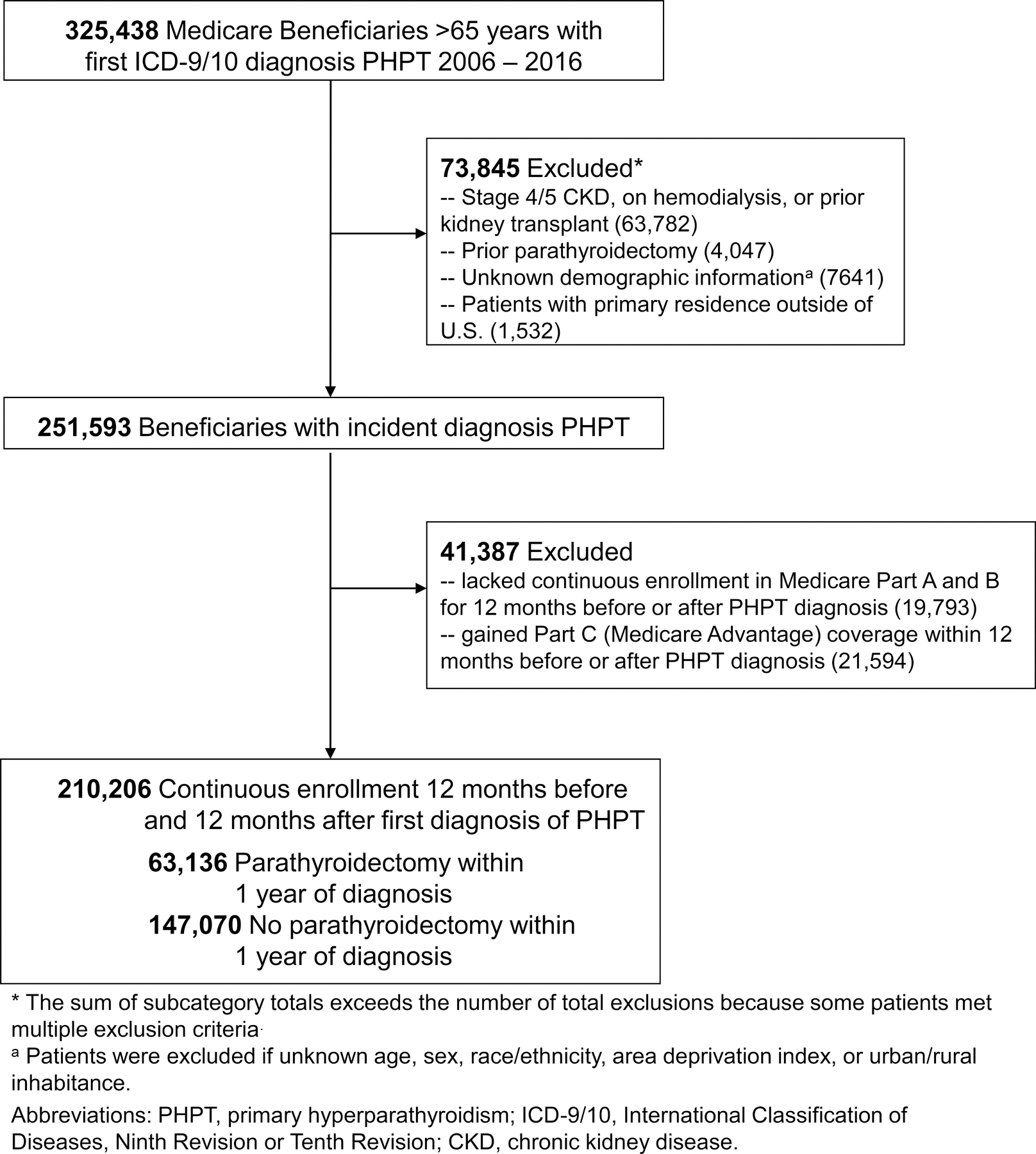
The authors conducted a population-based, longitudinal cohort study of Medicare beneficiaries diagnosed with PHPT (2006-2017). Multivariable, inverse probability weighted Cox proportional hazards regression was used to determine the associations of parathyroidectomy with major adverse cardiovascular events (MACEs), CV disease-related hospitalization, and CV hospitalization-associated mortality.
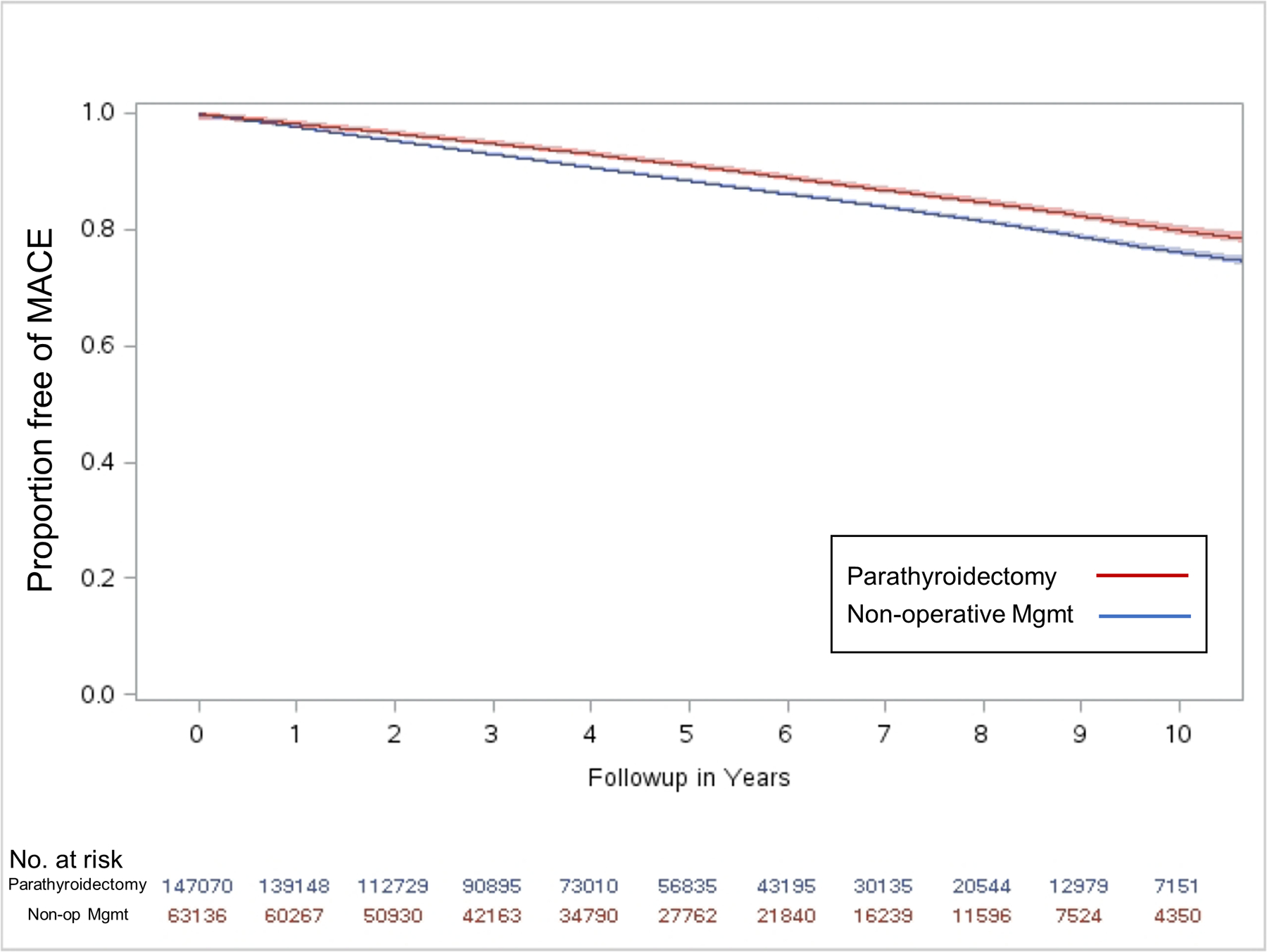
The authors identified 210,206 beneficiaries diagnosed with PHPT from 2006 to 2017. Among 63,136 (30.0%) treated with parathyroidectomy and 147,070 (70.0%) managed nonoperatively within 1 year of diagnosis, the unadjusted incidence of MACE was 10.0% [mean follow-up 59.1 (SD 35.6) months] and 11.5% [mean follow-up 54.1 (SD 34.0) months], respectively. In multivariable analysis, parathyroidectomy was associated with a lower incidence of MACE [hazard ratio (HR): 0.92; 95% confidence interval (95% CI): 0.90-0.94], CV disease-related hospitalization (HR: 0.89; 95% CI: 0.87-0.91), and CV hospitalization-associated mortality (HR: 0.76; 95% CI: 0.71-0.81) compared to nonoperative management. At 10 years, parathyroidectomy was associated with adjusted absolute risk reduction for MACE of 1.7% (95% CI: 1.3%-2.1%), for CV disease-related hospitalization of 2.5% (95% CI: 2.1%-2.9%), and for CV hospitalization-associated mortality of 1.4% (95% CI: 1.2%-1.6%).
In this large, population-based cohort study, parathyroidectomy was associated with a lower long-term incidence of adverse CV outcomes when compared with nonoperative management for older adults with PHPT, which is relevant to surgical decision making for patients with a long life expectancy.
作者旨在比较甲状旁腺功能亢进症(PHPT)老年患者接受甲状旁腺切除术与非手术治疗的不良心血管(CV)事件发生率。
PHPT 是一种常见的内分泌疾病,与 CV 死亡率增加有关,但尚不清楚甲状旁腺切除术是否能降低不良 CV 事件的发生率。
作者进行了一项基于人群的、纵向队列研究,纳入了 2006 年至 2017 年间被诊断为 PHPT 的医疗保险受益人群。采用多变量逆概率加权 Cox 比例风险回归来确定甲状旁腺切除术与主要不良心血管事件(MACE)、CV 疾病相关住院和 CV 住院相关死亡率的关系。
作者从 2006 年至 2017 年确定了 210206 名被诊断为 PHPT 的受益人群。在 63136 名(30.0%)接受甲状旁腺切除术治疗和 147070 名(70.0%)在诊断后 1 年内非手术治疗的患者中,未经调整的 MACE 发生率分别为 10.0%(平均随访 59.1 [35.6] 个月)和 11.5%(平均随访 54.1 [34.0] 个月)。多变量分析显示,与非手术治疗相比,甲状旁腺切除术与较低的 MACE 发生率相关[风险比(HR):0.92;95%置信区间(95%CI):0.90-0.94]、CV 疾病相关住院率(HR:0.89;95%CI:0.87-0.91)和 CV 住院相关死亡率(HR:0.76;95%CI:0.71-0.81)。10 年后,甲状旁腺切除术与 MACE 的调整绝对风险降低 1.7%(95%CI:1.3%-2.1%)、CV 疾病相关住院的调整绝对风险降低 2.5%(95%CI:2.1%-2.9%)和 CV 住院相关死亡率的调整绝对风险降低 1.4%(95%CI:1.2%-1.6%)相关。
在这项大型的基于人群的队列研究中,与 PHPT 老年患者的非手术治疗相比,甲状旁腺切除术与较低的长期不良 CV 结局发生率相关,这与预期寿命较长的患者的手术决策相关。