Jesinghaus Moritz, Poppinga Jelte, Lehman Bettina, Maurer Elisabeth, Ramaswamy Annette, Grass Albert, Di Fazio Pietro, Rinke Anja, Denkert Carsten, Bartsch Detlef K
Institute of Pathology, Phillips University Marburg and University Hospital Marburg, 35043 Marburg, Germany.
Department of Visceral, Thoracic and Vascular Surgery, Phillips University Marburg and University Hospital Marburg, 35043 Marburg, Germany.
Cancers (Basel). 2022 Aug 17;14(16):3963. doi: 10.3390/cancers14163963.
A recent study found that multifocal jejunoileal neuroendocrine tumors (SI-NETs) are genetically unrelated synchronous neoplasms. So far, it is unclear if this finding of synchronous independent neoplasms is mirrored by heterogeneity of key morphological parameters of SI-NETs and how it affects patient survival.
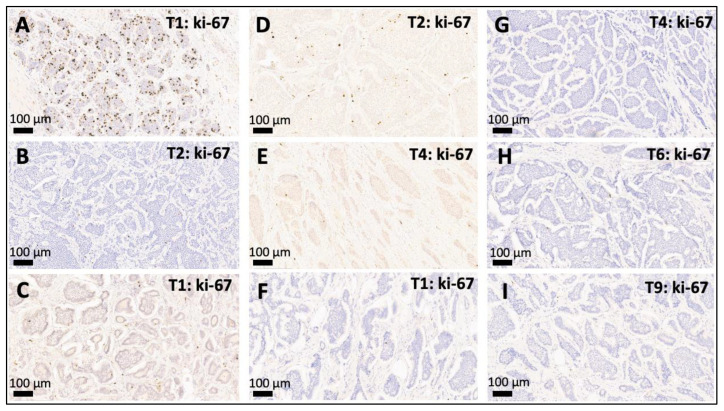
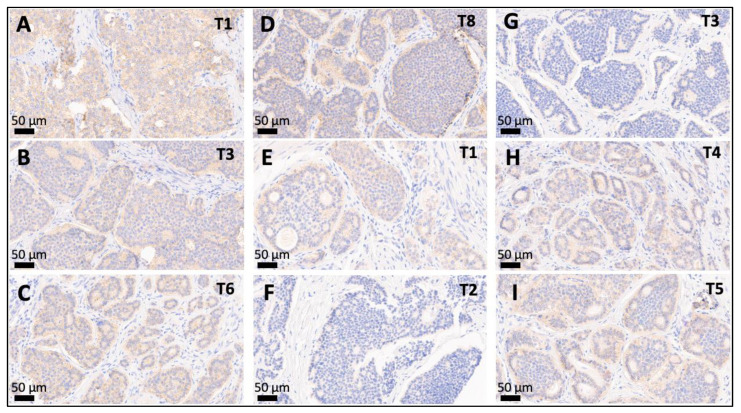
We separately assessed WHO grade (based on the Ki-67 index), expression of basal diagnostic markers (synaptophysin/chromogranin A/CDX2/serotonin), SSTR2a, and the contexture of the immunogenic microenvironment in 146 separate tumors from 28 patients with multifocal SI-NETs and correlated the results with clinicopathological factors and survival.
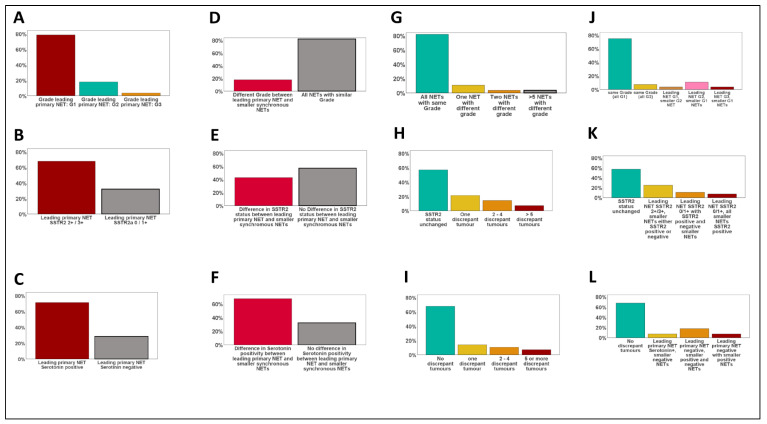
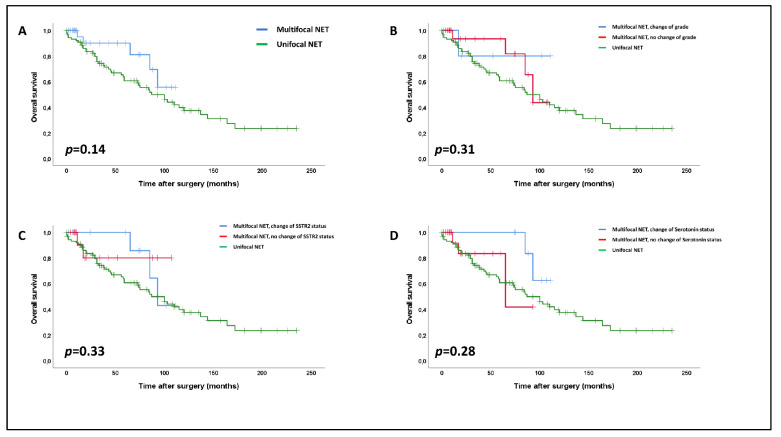
Synaptophysin and chromogranin A were strongly expressed in all tumors. WHO grade was concordant within all multifocal lesions in more than 80% of cases and the highest grade was usually found in the most advanced primary. Intertumoral expression of serotonin, SSTR2, and CDX2 was discrepant in 32%, 43%, and 50% of all patients, respectively. Neither heterogeneity of any of the aforementioned markers nor multifocality itself had any impact on patient survival ( = n.s.).
Multifocal SI-NET show considerable variability in some of the central diagnostic parameters. However, neither intertumoral heterogeneity of those parameters nor multifocality itself had any impact on patient survival, showing that extensive testing of all multifocal lesions is not necessarily required.
最近一项研究发现,多灶性空肠回肠神经内分泌肿瘤(SI-NETs)是基因不相关的同步性肿瘤。到目前为止,尚不清楚同步性独立肿瘤这一发现是否反映在SI-NETs关键形态学参数的异质性上,以及它如何影响患者生存。
我们分别评估了28例多灶性SI-NETs患者的146个独立肿瘤的WHO分级(基于Ki-67指数)、基础诊断标志物(突触素/嗜铬粒蛋白A/CDX2/血清素)的表达、SSTR2a以及免疫原性微环境的结构,并将结果与临床病理因素和生存情况相关联。
所有肿瘤中突触素和嗜铬粒蛋白A均呈强表达。在超过80%的病例中,所有多灶性病变内的WHO分级是一致的,最高分级通常见于最晚期的原发灶。血清素、SSTR2和CDX2的肿瘤间表达差异分别在所有患者的32%、43%和50%中出现。上述任何标志物的异质性以及多灶性本身均对患者生存无任何影响(P = 无统计学意义)。
多灶性SI-NET在一些核心诊断参数上显示出相当大的变异性。然而,这些参数的肿瘤间异质性以及多灶性本身均对患者生存无任何影响,表明不一定需要对所有多灶性病变进行广泛检测。