Gastroenterology Department, Cochin Hospital, Assistance Publique - Hôpitaux de Paris, 27 rue du Faubourg Saint Jacques, 75014, Paris, France.
Université de Paris Cité, Paris, France.
Sci Rep. 2022 Aug 26;12(1):14592. doi: 10.1038/s41598-022-18528-7.
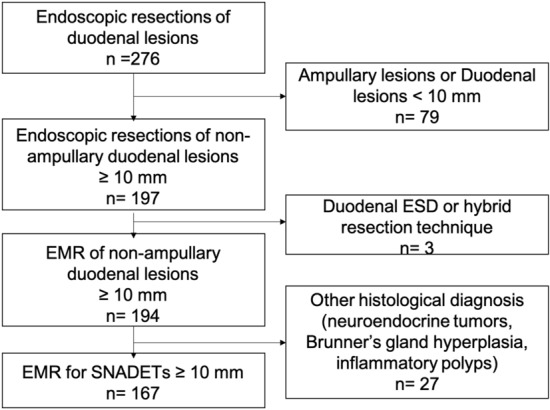
Endoscopic mucosal resection (EMR) is the recommended treatment for superficial non-ampullary duodenal epithelial tumors larger than 6 mm. This endoscopic technique carries a high risk of adverse events. Our aim was to identify the risk factors for adverse events following EMR for non-ampullary duodenal adenomatous lesions. We retrospectively analyzed a prospectively collected database of consecutive endoscopic resections for duodenal lesions at a tertiary referral center for therapeutic endoscopy. We analyzed patients with non-ampullary duodenal adenomatous lesions ≥ 10 mm resected by EMR, and searched for factors associated with adverse events after EMR. 167 duodenal adenomatous lesions, with a median size of 25 (25-40) mm, were resected by EMR between January 2015 and December 2020. Adverse events occurred in 37/167 (22.2%) after endoscopic resection, with 29/167 (17.4%) delayed bleeding, 4/167 (2.4%) immediate perforation and 4/167 (2.4%) delayed perforation. In logistic regression, the size of the lesion was the only associated risk factor of adverse events (OR = 2.81, 95% CI [1.27; 6.47], p = 0.012). Adverse events increased mean hospitalization time (7.7 ± 9 vs. 1.9 ± 1 days, p < 0.01). None of the currently recommended preventive methods, particularly clips, affected the adverse event rate. EMR of centimetric and supracentimetric duodenal adenomatous lesions carries a high risk of adverse events, increasing with the size of the lesion and with no benefit from any preventive method. These results suggest that these procedures should be performed in expert centers, and underline the need for novel endoscopic tools to limit the rate of adverse events.
内镜黏膜切除术(EMR)是治疗直径大于 6 毫米的非壶腹性十二指肠上皮性肿瘤的推荐方法。这种内镜技术具有很高的不良事件风险。我们的目的是确定非壶腹性十二指肠腺瘤性病变行 EMR 后发生不良事件的危险因素。我们对一家治疗性内镜转诊中心连续内镜切除十二指肠病变的前瞻性数据库进行了回顾性分析。我们分析了经 EMR 切除的直径≥10 毫米的非壶腹性十二指肠腺瘤性病变患者,并寻找与 EMR 后不良事件相关的因素。2015 年 1 月至 2020 年 12 月,我们共切除了 167 个十二指肠腺瘤性病变,中位数大小为 25(25-40)毫米。内镜切除后,37/167(22.2%)发生不良事件,其中 29/167(17.4%)为延迟性出血,4/167(2.4%)为即刻穿孔,4/167(2.4%)为延迟性穿孔。在 logistic 回归中,病变的大小是唯一与不良事件相关的危险因素(OR=2.81,95%CI[1.27;6.47],p=0.012)。不良事件增加了平均住院时间(7.7±9 天 vs. 1.9±1 天,p<0.01)。目前推荐的预防方法,特别是夹闭,均未影响不良事件的发生率。厘米级和超厘米级十二指肠腺瘤性病变行 EMR 有较高的不良事件风险,其风险随病变大小增加而增加,且任何预防方法均无获益。这些结果表明,这些操作应在有经验的中心进行,并强调需要新的内镜工具来降低不良事件的发生率。