University of Colorado School of Medicine, Aurora, Colorado, USA.
Faculty of Medicine and Health Sciences, University of Zimbabwe, Harare, Zimbabwe.
J Int AIDS Soc. 2022 Aug;25(8):e25998. doi: 10.1002/jia2.25998.
Most Zimbabweans access medical care through tiered health systems. In 2013, HIV care was decentralized to primary care clinics; while oncology care remained centralized. Most persons in Zimbabwe with Kaposi sarcoma (KS) are diagnosed late in their disease, and the prognosis is poor. Little is known about whether educational interventions could improve KS outcomes in these settings.
Interventions to improve KS detection and management were evaluated at eight Zimbabwe primary care sites (four rural/four urban) that provided HIV care. Interventions included a standardized KS clinical evaluation tool, palliative care integration, standardized treatment and improved consultative services. Interventions were implemented between February 2013 and January 2016 using a randomized stepped-wedge cluster design. Sites were monitored for KS diagnosis rates and KS outcomes, including early diagnosis (T0 vs. T1 tumour stage), participant retention and mortality. Analyses controlled for within-clinic correlations.
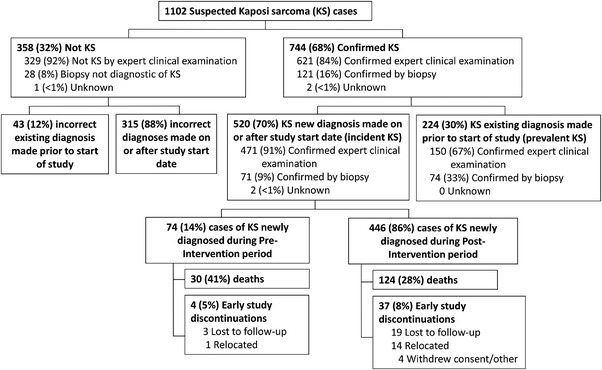
A total of 1102 persons with suspected KS (96% HIV positive) were enrolled: 47% incident (new diagnosis), 20% prevalent (previous diagnosis) and 33% determined as not KS. Early (T0) diagnosis increased post-intervention, though not significant statistically (adjusted odds ratio [aOR] = 1.48 [95% confidence interval (95% CI): 0.66-3.79], p = 0.37). New KS diagnosis rates increased 103% (95% CI: 11-273%), p = 0.02) post-intervention; although paired with an increased odds of incorrectly diagnosing KS (aOR = 2.08 [95% CI: 0.33-3.24], p = 0.001). Post-intervention, non-significant decreases in 90-day return rates (adjusted hazard ratio [aHR] = 0.69 [95% CI: 0.38-1.45], p = 0.21) and survival (aHR = 1.36 [95% CI: 0.85-2.20], p = 0.20) were estimated.
KS training interventions at urban and rural Zimbabwe decentralized primary care clinics significantly increased overall and incorrect KS diagnosis rates, but not early KS diagnosis rates, 90-day return rates or survival.
大多数津巴布韦人通过分层医疗系统获得医疗服务。2013 年,艾滋病毒治疗工作已下放至初级保健诊所;而肿瘤治疗仍集中于中心医院。津巴布韦大多数卡波西肉瘤(KS)患者在疾病晚期才被诊断出来,预后较差。关于教育干预措施是否能改善这些环境下 KS 的预后,目前知之甚少。
在提供艾滋病毒护理的津巴布韦八个初级保健点(4 个农村/4 个城市)评估了改善 KS 检测和管理的干预措施。这些干预措施包括使用标准化 KS 临床评估工具、姑息治疗整合、标准化治疗和改善咨询服务。干预措施于 2013 年 2 月至 2016 年 1 月期间采用随机分阶段楔形集群设计实施。对各医疗点 KS 诊断率和 KS 结局进行监测,包括早期诊断(T0 期与 T1 期肿瘤分期)、参与者保留率和死亡率。分析时控制了诊所内相关性。
共纳入 1102 例疑似 KS 患者(96% HIV 阳性):47%为新发病例(新诊断),20%为现患病例(以前诊断),33%为非 KS 病例。干预后早期(T0)诊断增加,但无统计学意义(校正比值比[aOR] = 1.48[95%可信区间(95%CI):0.66-3.79],p = 0.37)。新 KS 诊断率增加 103%(95%CI:11-273%),p = 0.02);但 KS 误诊的几率也相应增加(校正比值比[aOR] = 2.08[95%CI:0.33-3.24],p = 0.001)。干预后,90 天内复诊率(校正风险比[aHR] = 0.69[95%CI:0.38-1.45],p = 0.21)和生存率(aHR = 1.36[95%CI:0.85-2.20],p = 0.20)的降低均无统计学意义。
在津巴布韦城乡的初级保健诊所开展 KS 培训干预措施显著增加了整体和错误 KS 诊断率,但并未增加早期 KS 诊断率、90 天内复诊率或生存率。