Lang Hervé, Béraud Claire, Cabel Luc, Fontugne Jacqueline, Lassalle Myriam, Krucker Clémentine, Dufour Florent, Groeneveld Clarice S, Dixon Victoria, Meng Xiangyu, Kamoun Aurélie, Chapeaublanc Elodie, De Reynies Aurélien, Gamé Xavier, Rischmann Pascal, Bieche Ivan, Masliah-Planchon Julien, Beaurepere Romane, Allory Yves, Lindner Véronique, Misseri Yolande, Radvanyi François, Lluel Philippe, Bernard-Pierrot Isabelle, Massfelder Thierry
Department of Urology, New Civil Hospital and Fédération de Médecine Translationnelle de Strasbourg (FMTS), Strasbourg, France.
Urosphere, Toulouse, France.
Front Oncol. 2022 Aug 11;12:930731. doi: 10.3389/fonc.2022.930731. eCollection 2022.
Muscle-invasive bladder cancer (MIBC) and upper urinary tract urothelial carcinoma (UTUC) are molecularly heterogeneous. Despite chemotherapies, immunotherapies, or anti-fibroblast growth factor receptor (FGFR) treatments, these tumors are still of a poor outcome. Our objective was to develop a bank of patient-derived xenografts (PDXs) recapitulating the molecular heterogeneity of MIBC and UTUC, to facilitate the preclinical identification of therapies.
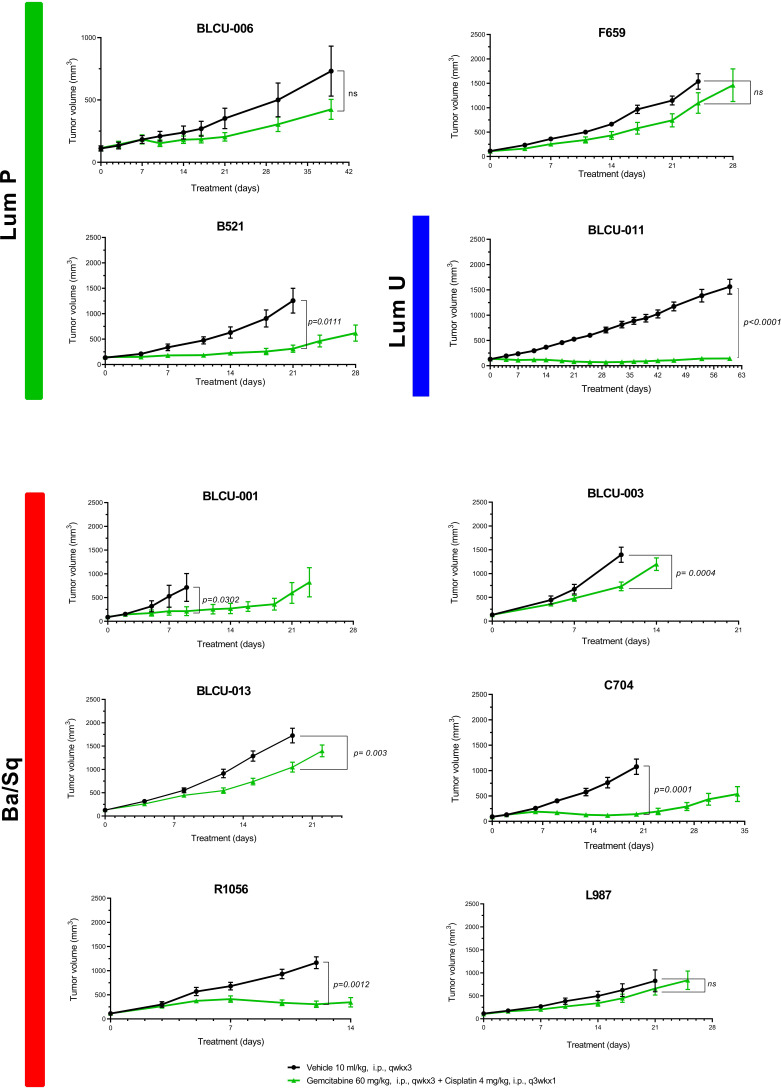
Fresh tumors were obtained from patients and subcutaneously engrafted into immune-compromised mice. Patient tumors and matched PDXs were compared regarding histopathology, transcriptomic (microarrays), and genomic profiles [targeted Next-Generation Sequencing (NGS)]. Several PDXs were treated with chemotherapy (cisplatin/gemcitabine) or targeted therapies [FGFR and epidermal growth factor (EGFR) inhibitors].
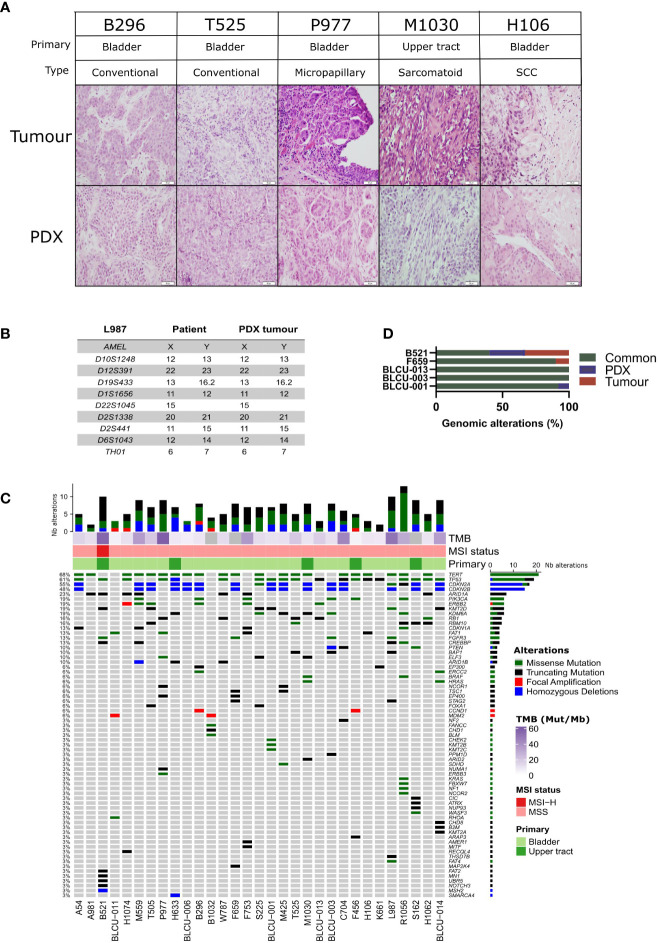
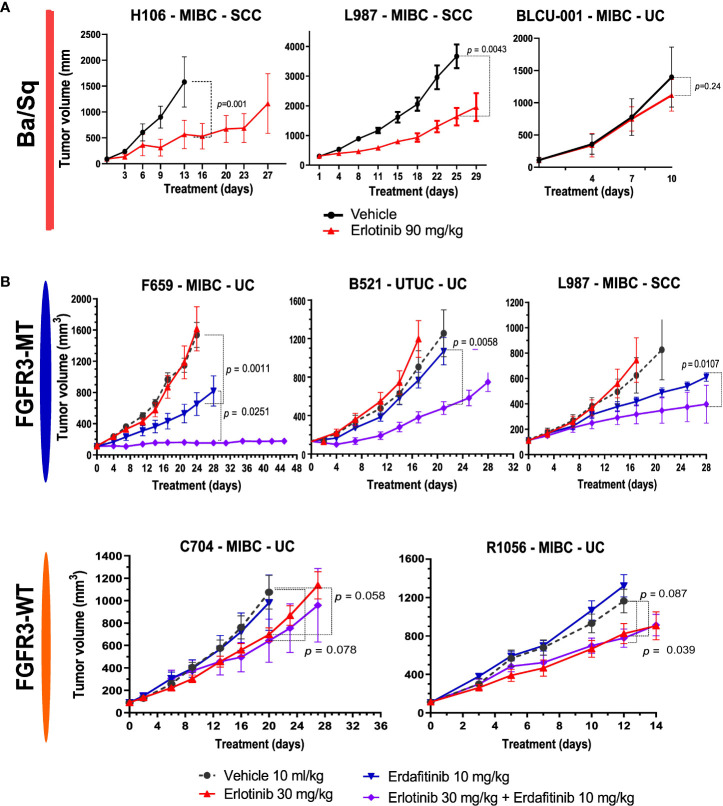
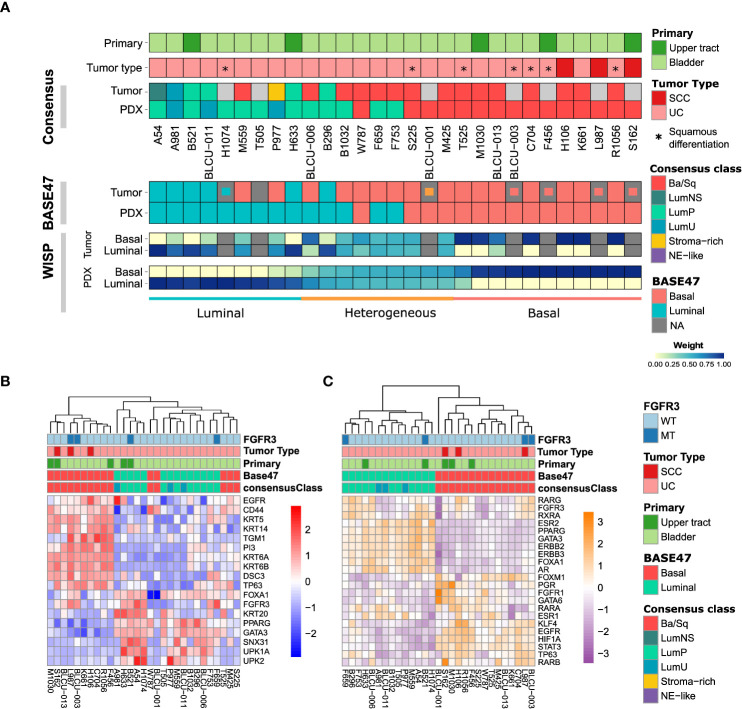
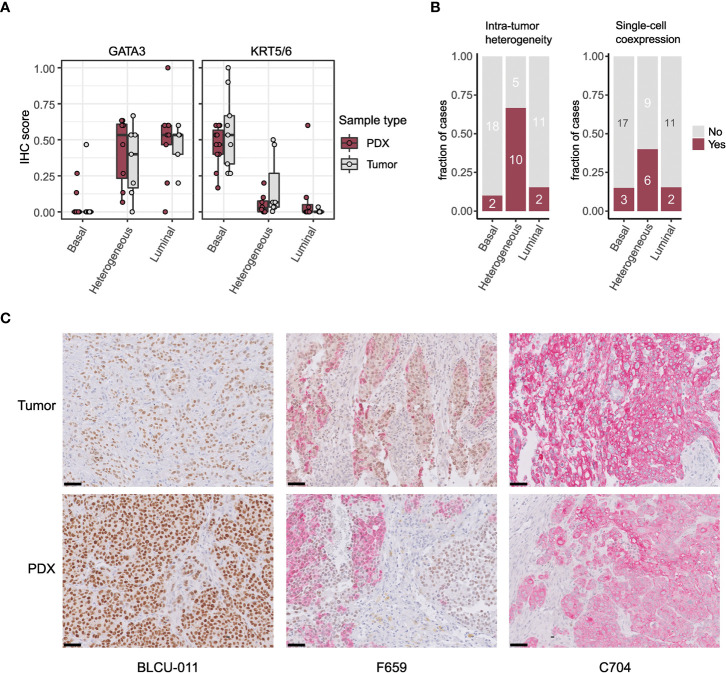
A total of 31 PDXs were established from 1 non-MIBC, 25 MIBC, and 5 upper urinary tract tumors, including 28 urothelial (UC) and 3 squamous cell carcinomas (SCCs). Integrated genomic and transcriptomic profiling identified the PDXs of three different consensus molecular subtypes [basal/squamous (Ba/Sq), luminal papillary, and luminal unstable] and included -mutated PDXs. High histological and genomic concordance was found between matched patient tumor/PDX. Discordance in molecular subtypes, such as a Ba/Sq patient tumor giving rise to a luminal papillary PDX, was observed (n=5) at molecular and histological levels. Ten models were treated with cisplatin-based chemotherapy, and we did not observe any association between subtypes and the response. Of the three Ba/Sq models treated with anti-EGFR therapy, two models were sensitive, and one model, of the sarcomatoid variant, was resistant. The treatment of three FGFR3-mutant PDXs with combined FGFR/EGFR inhibitors was more efficient than anti-FGFR3 treatment alone.
We developed preclinical PDX models that recapitulate the molecular heterogeneity of MIBCs and UTUC, including actionable mutations, which will represent an essential tool in therapy development. The pharmacological characterization of the PDXs suggested that the upper urinary tract and MIBCs, not only UC but also SCC, with similar molecular characteristics could benefit from the same treatments including anti-FGFR for FGFR3-mutated tumors and anti-EGFR for basal ones and showed a benefit for combined FGFR/EGFR inhibition in FGFR3-mutant PDXs, compared to FGFR inhibition alone.
肌层浸润性膀胱癌(MIBC)和上尿路尿路上皮癌(UTUC)在分子层面具有异质性。尽管有化疗、免疫疗法或抗成纤维细胞生长因子受体(FGFR)治疗,但这些肿瘤的预后仍然很差。我们的目标是建立一组能重现MIBC和UTUC分子异质性的患者来源异种移植瘤(PDX)库,以促进临床前治疗方法的鉴定。
从患者处获取新鲜肿瘤,并皮下移植到免疫缺陷小鼠体内。对患者肿瘤和匹配的PDX进行组织病理学、转录组学(微阵列)和基因组图谱[靶向新一代测序(NGS)]比较。对几个PDX进行化疗(顺铂/吉西他滨)或靶向治疗[FGFR和表皮生长因子(EGFR)抑制剂]。
共从1例非MIBC、25例MIBC和5例上尿路肿瘤中建立了31个PDX,包括28例尿路上皮癌(UC)和3例鳞状细胞癌(SCC)。综合基因组和转录组分析确定了三种不同的共识分子亚型[基底/鳞状(Ba/Sq)、腔面乳头状和腔面不稳定]的PDX,并包括有突变的PDX。在匹配的患者肿瘤/PDX之间发现了高度的组织学和基因组一致性。在分子和组织学水平上观察到分子亚型的不一致,例如Ba/Sq患者肿瘤产生了腔面乳头状PDX(n = 5)。对10个模型进行了基于顺铂的化疗,我们未观察到亚型与反应之间的任何关联。在用抗EGFR治疗的三个Ba/Sq模型中,两个模型敏感,而一个肉瘤样变体模型耐药。用FGFR/EGFR联合抑制剂治疗三个FGFR3突变的PDX比单独使用抗FGFR3治疗更有效。
我们建立了临床前PDX模型,该模型重现了MIBC和UTUC的分子异质性,包括可操作的突变,这将成为治疗开发中的重要工具。PDX的药理学特征表明,具有相似分子特征的上尿路和MIBC,不仅是UC,还有SCC,可从相同的治疗中获益,包括对FGFR3突变肿瘤使用抗FGFR治疗,对基底型肿瘤使用抗EGFR治疗,并且与单独使用FGFR抑制相比,FGFR3突变的PDX联合使用FGFR/EGFR抑制显示出益处。