Division of Hematology, Department of Medicine, University of North Carolina School of Medicine, Chapel Hill, NC.
UNC Blood Research Center, University of North Carolina School of Medicine, Chapel Hill, NC.
Blood Adv. 2023 Mar 28;7(6):900-908. doi: 10.1182/bloodadvances.2022008255.
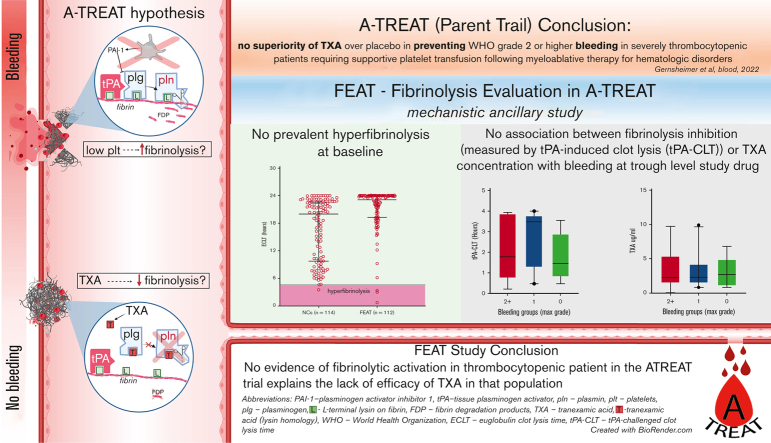
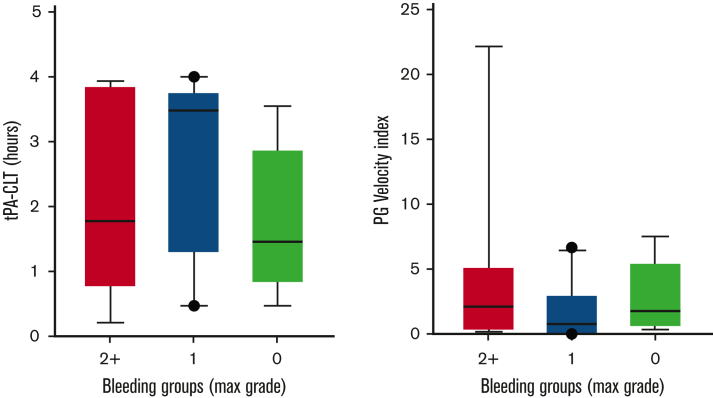
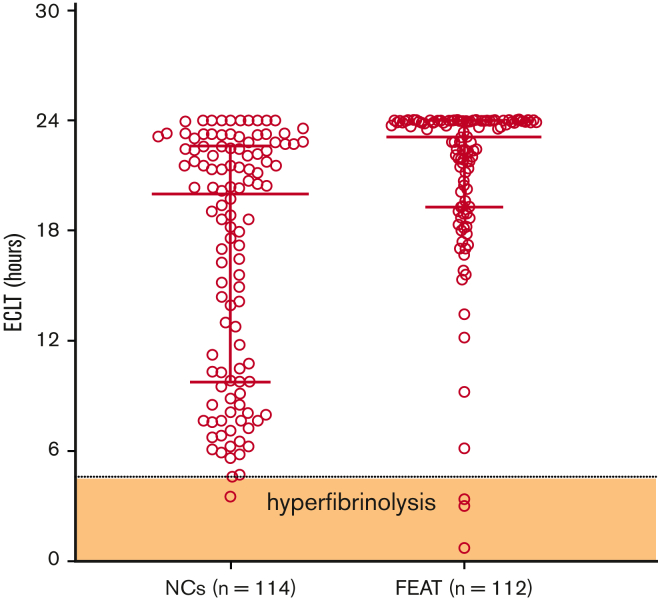
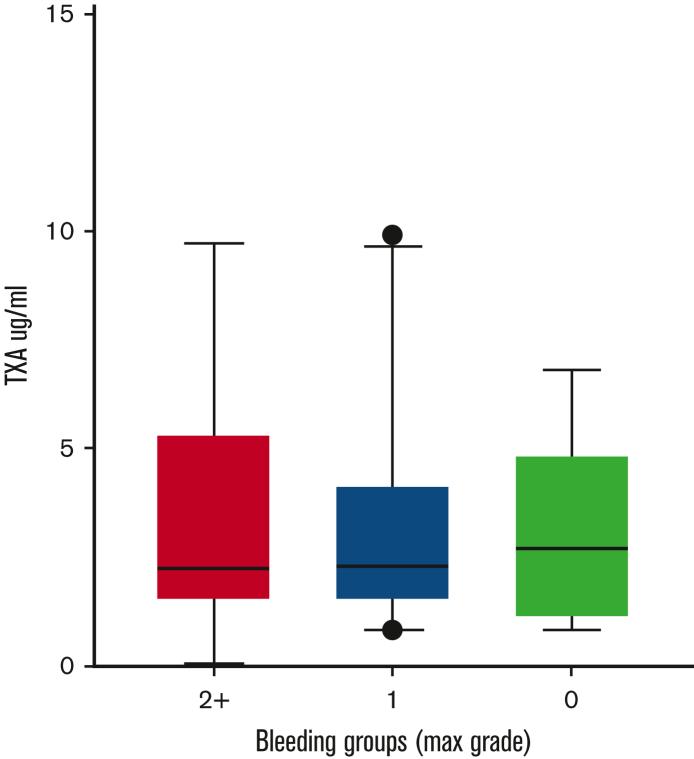
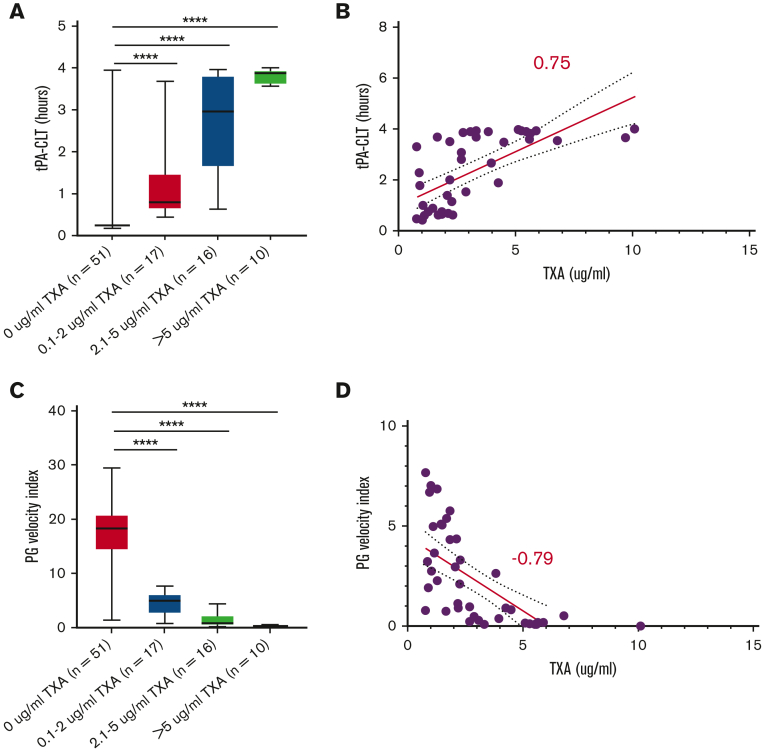
The American Trial Using Tranexamic Acid (TXA) in Thrombocytopenia (A-TREAT, NCT02578901) demonstrated no superiority of TXA over placebo in preventing World Health Organization (WHO) grade 2 or higher bleeding in patients with severe thrombocytopenia requiring supportive platelet transfusion following myeloablative therapy for hematologic disorders. In this ancillary study, we sought to determine whether this clinical outcome could be explained on the basis of correlative assays of fibrinolysis. Plasma was collected from A-TREAT participants (n = 115) before the initiation of study drug (baseline) and when TXA was at steady-state trough concentration (follow-up). Global fibrinolysis was measured by 3 assays: euglobulin clot lysis time (ECLT), plasmin generation (PG), and tissue-type plasminogen activator (tPA)-challenged clot lysis time (tPA-CLT). TXA was quantified in follow-up samples by tandem mass spectrometry. Baseline samples did not demonstrate fibrinolytic activation by ECLT or tPA-CLT. Furthermore, neither ECLT nor levels of plasminogen activator inhibitor-1, tPA, plasminogen, alpha2-antiplasmin, or plasmin-antiplasmin complexes were associated with a greater risk of WHO grade 2+ bleeding. TXA trough concentrations were highly variable (range, 0.7-10 μg/mL) and did not correlate with bleeding severity, despite the fact that plasma TXA levels correlated strongly with pharmacodynamic assessments by PG (Spearman r, -0.78) and tPA-CLT (r, 0.74). We conclude that (1) no evidence of fibrinolytic activation was observed in these patients with thrombocytopenia, (2) trough TXA concentrations varied significantly between patients receiving the same dosing schedule, and (3) tPA-CLT and PG correlated well with TXA drug levels.
美国的一项使用氨甲环酸(TXA)治疗血小板减少症的试验(A-TREAT,NCT02578901)表明,在接受骨髓清除性治疗后需要支持性血小板输注以治疗严重血小板减少症的患者中,与安慰剂相比,TXA 并不能预防世界卫生组织(WHO)2 级或更高级别的出血。在这项辅助研究中,我们试图确定这种临床结果是否可以根据纤溶相关检测来解释。从 A-TREAT 参与者(n=115)中采集研究药物开始前(基线)和 TXA 达到稳定谷浓度时(随访)的血浆。通过 3 种检测方法测量整体纤溶:优球蛋白溶解时间(ECLT)、纤溶酶原生成(PG)和组织型纤溶酶原激活物(tPA)挑战的纤维蛋白溶解时间(tPA-CLT)。通过串联质谱法在随访样本中定量测定 TXA。基线样本未通过 ECLT 或 tPA-CLT 显示纤溶激活。此外,ECLT 或纤溶酶原激活物抑制剂-1、tPA、纤溶酶原、α2-抗纤溶酶或纤溶酶-抗纤溶酶复合物的水平均与 WHO 2+级出血风险增加无关。尽管事实上,血浆 TXA 水平与 PG(Spearman r,-0.78)和 tPA-CLT(r,0.74)的药效学评估密切相关,但 TXA 谷浓度的变异性很大(范围为 0.7-10μg/mL),且与出血严重程度无关。我们得出结论:(1)在这些血小板减少症患者中未观察到纤溶激活的证据;(2)接受相同给药方案的患者之间的 TXA 谷浓度差异很大;(3)tPA-CLT 和 PG 与 TXA 药物水平相关性良好。