Department of Paediatrics and Child Health, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Princess of Wales Terrace, Parktown, Johannesburg, 2193, South Africa.
Paediatric Gastroenterology, Hepatology and Nutrition Unit, Charlotte Maxeke Johannesburg Academic Hospital, University of Witwatersrand, Johannesburg, South Africa.
BMC Pediatr. 2022 Aug 31;22(1):516. doi: 10.1186/s12887-022-03574-x.
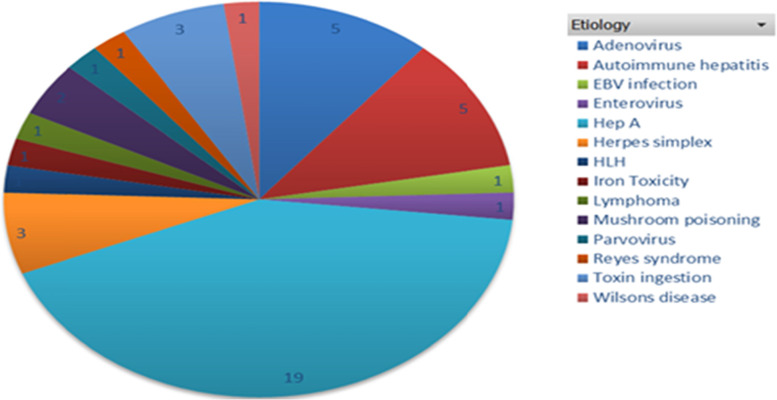
Pediatric acute liver failure (PALF) is an uncommon, devastating illness with significant mortality. Liver transplantation remains the mainstay of treatment for irreversible PALF. The purpose of this study was to determine the etiology and prognostic factors associated with outcome of PALF in South Africa and to evaluate prognostic scoring systems used.
Records of 45 pediatric patients younger than 16 years of age who presented with PALF from 1 January 2015 till 31 October 2020 were analysed. Patients were divided into two groups with one group consisting of patients with spontaneous recovery of the liver with supportive treatment (6/45:13.3%) and the second group consisting of patients with poor outcomes who demised (19/45: 42%) or underwent liver transplantation (20/45: 44%).
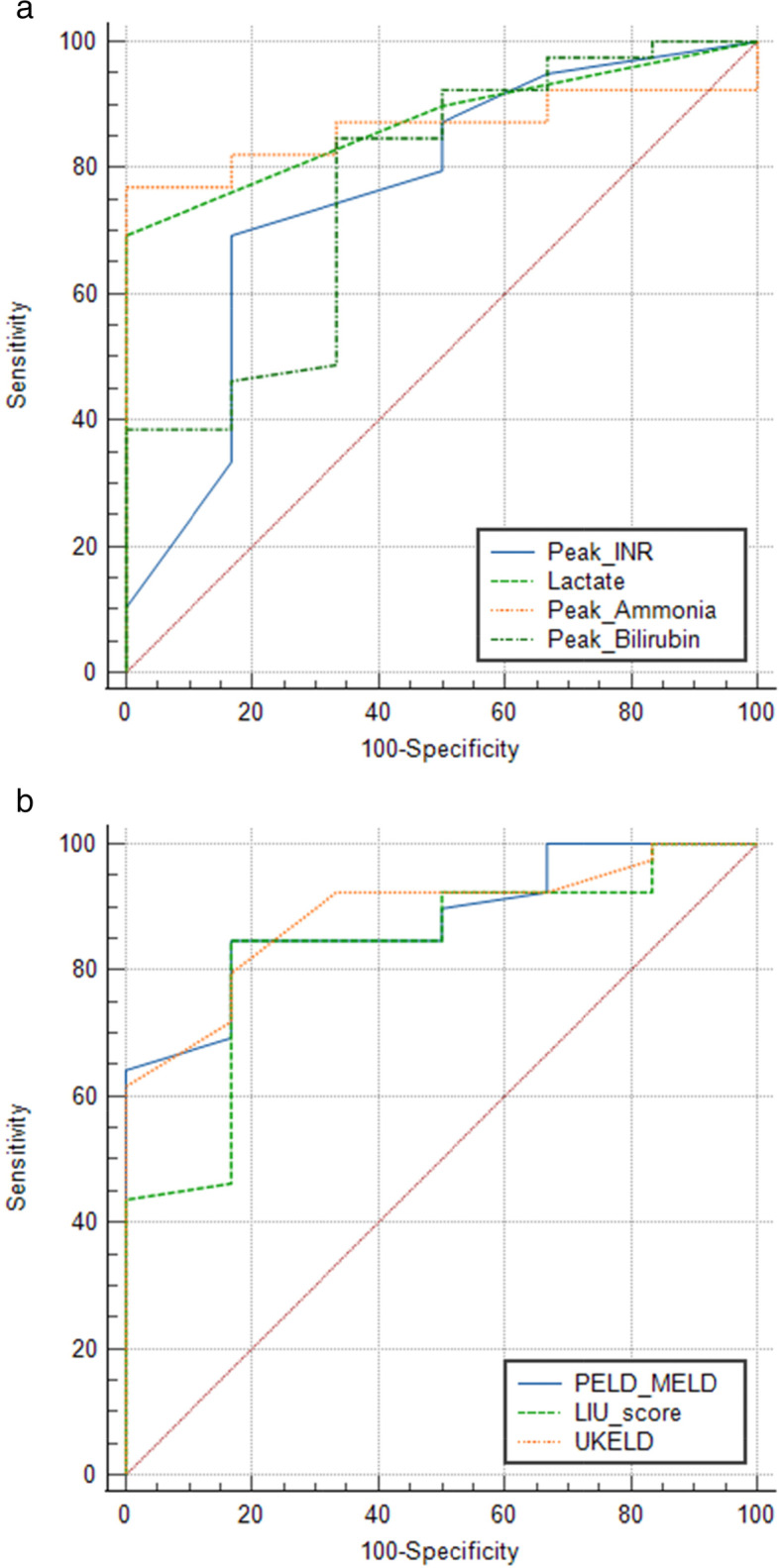
The median age of presentation was 3.3 years (IQR 1.8-6.9) with the 1-5 years age group constituting majority of patients (55.6%). Median time to follow up was 6.1 months (IQR 0.2-28.8). Higher liver injury unit scores were observed in patients who had poorer outcomes (P = 0.008) with a threshold of greater than 246 having a sensitivity of 84% and specificity of 83% (P < 0.001). Higher peak PELD/MELD (P = 0.006) and admission UKELD (P = 0.002) scores, were found in patients with poorer outcomes. Kings College Hospital criteria (KCHC) was useful in predicting which patients would die without liver transplantation (P = 0.002). Liver transplantation was performed in 20/45 (44%) patients with a post transplantation 1 year patient and graft survival of 80%.
Although, survival of PALF patients was lower than high and other low-middle income countries, outcomes post transplantation were good. Our study demonstrates the utility of dynamic scoring systems in PALF patients, it underscores the need for early referral and clinical monitoring in a tertiary center once the criteria for PALF have been met.
小儿急性肝衰竭(PALF)是一种罕见的、毁灭性的疾病,死亡率很高。肝移植仍然是治疗不可逆性 PALF 的主要方法。本研究的目的是确定南非 PALF 的病因和预后因素,并评估使用的预后评分系统。
分析了 2015 年 1 月 1 日至 2020 年 10 月 31 日期间因 PALF 就诊的 45 名 16 岁以下儿科患者的记录。将患者分为两组,一组为接受支持治疗后肝脏自发恢复的患者(6/45:13.3%),另一组为预后不良的患者,包括死亡(19/45:42%)或接受肝移植(20/45:44%)的患者。
中位就诊年龄为 3.3 岁(IQR 1.8-6.9),1-5 岁年龄组占多数(55.6%)。中位随访时间为 6.1 个月(IQR 0.2-28.8)。预后不良的患者肝损伤单位评分较高(P=0.008),评分大于 246 的患者灵敏度为 84%,特异性为 83%(P<0.001)。更高的峰值 PELD/MELD(P=0.006)和入院 UKELD(P=0.002)评分见于预后不良的患者。金斯学院医院标准(KCHC)有助于预测哪些患者在没有肝移植的情况下会死亡(P=0.002)。20/45(44%)名患者接受了肝移植,移植后 1 年患者和移植物的存活率为 80%。
尽管 PALF 患者的生存率低于高收入和其他中低收入国家,但移植后结局良好。我们的研究表明,动态评分系统在 PALF 患者中的应用具有实用性,它强调了一旦符合 PALF 的标准,就需要在三级中心进行早期转诊和临床监测。