Department of Cardiac Surgery, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, Calif.
Department of Cardiac Surgery, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, Calif.
J Thorac Cardiovasc Surg. 2023 May;165(5):1849-1860.e6. doi: 10.1016/j.jtcvs.2022.05.005. Epub 2022 May 15.
Heart donation after circulatory death was recently reintroduced in the United States with hopes of increasing donor heart availability. We examined its national use and outcomes.
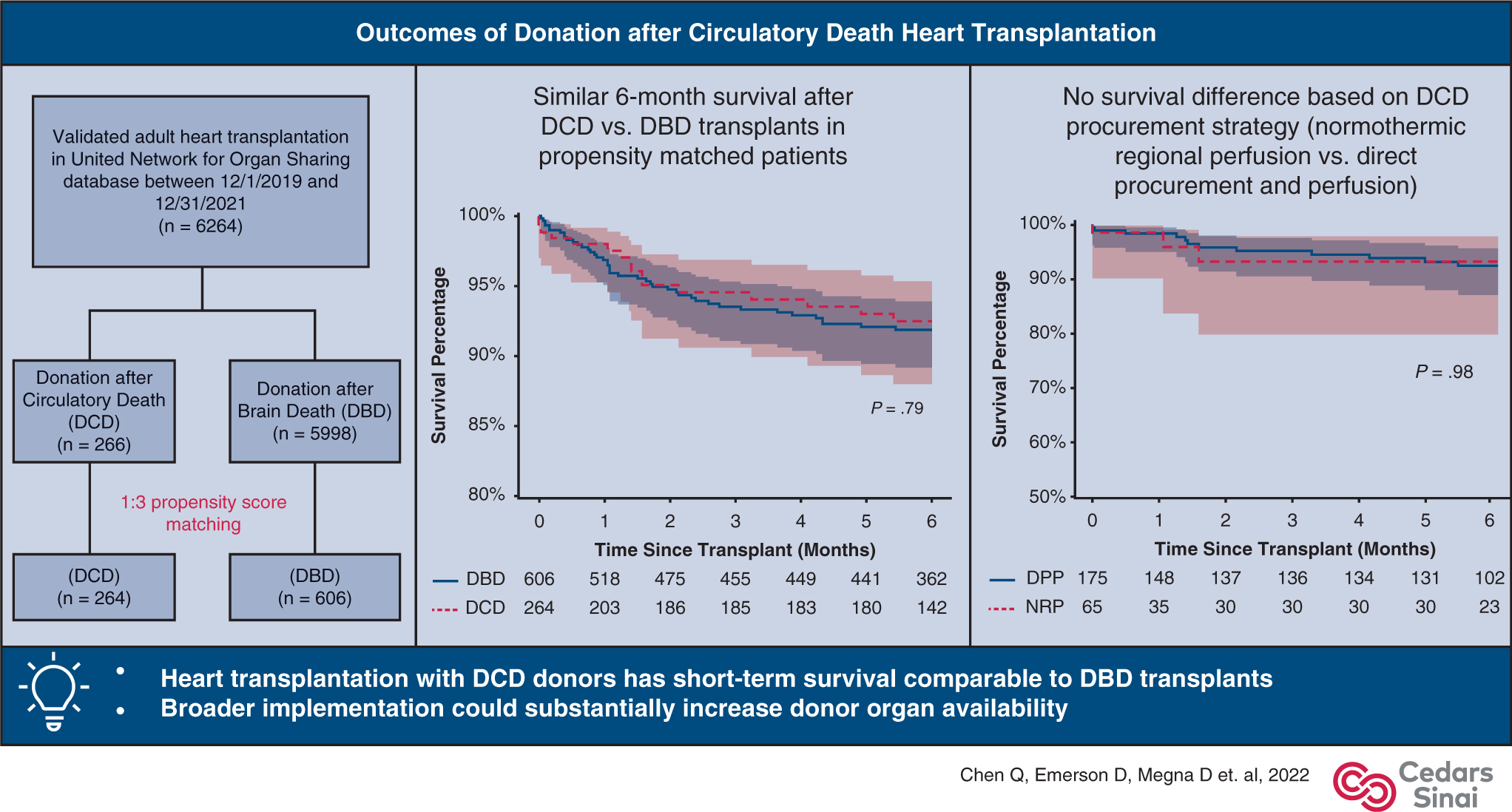
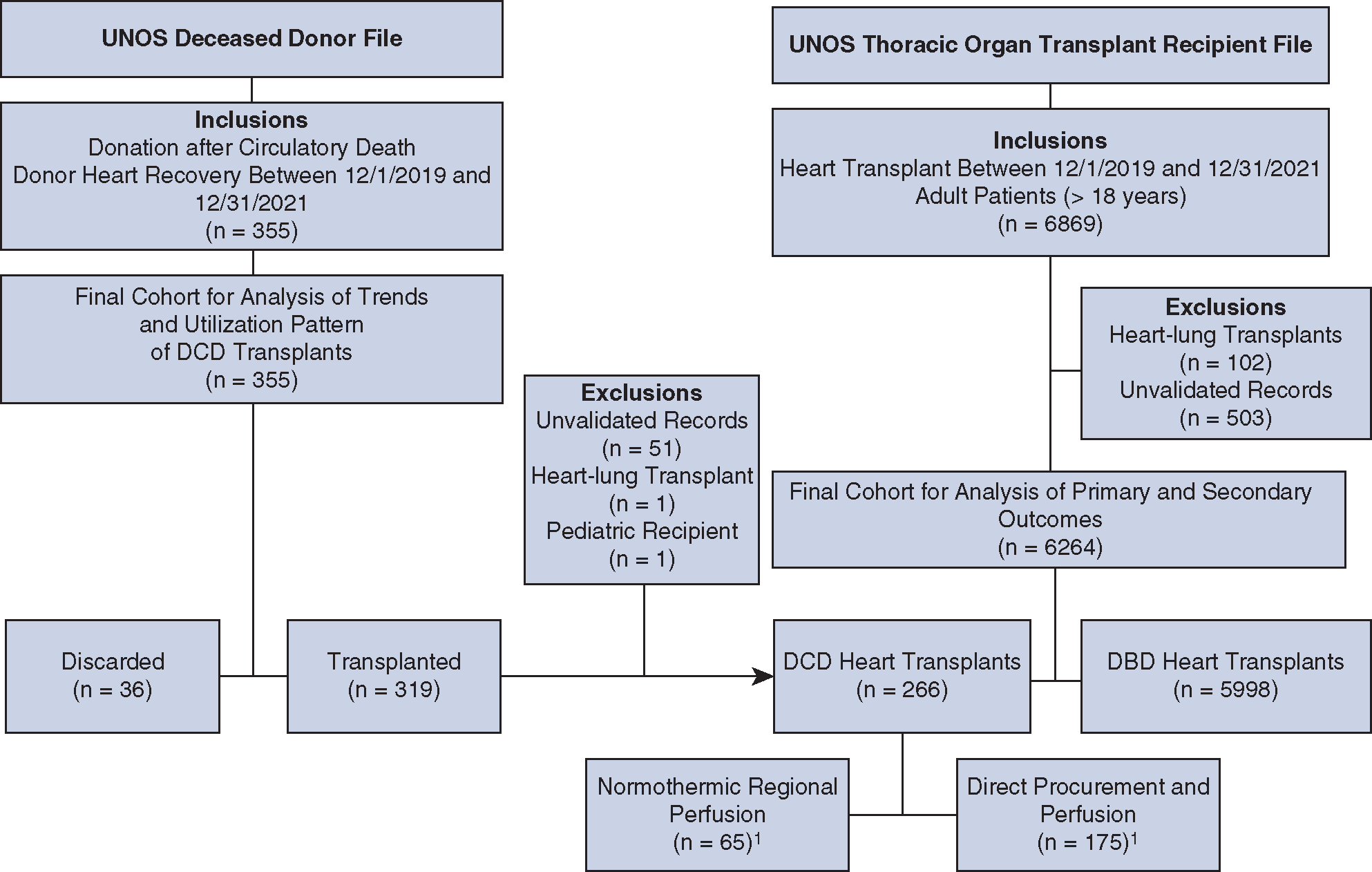
The United Network for Organ Sharing database was used to identify validated adult patients undergoing heart transplantation using donation after circulatory death donors (n = 266) and donation after brain death donors (n = 5998) between December 1, 2019, and December 31, 2021, after excluding heart-lung transplants. Propensity score matching was used to create more balanced groups for comparison.
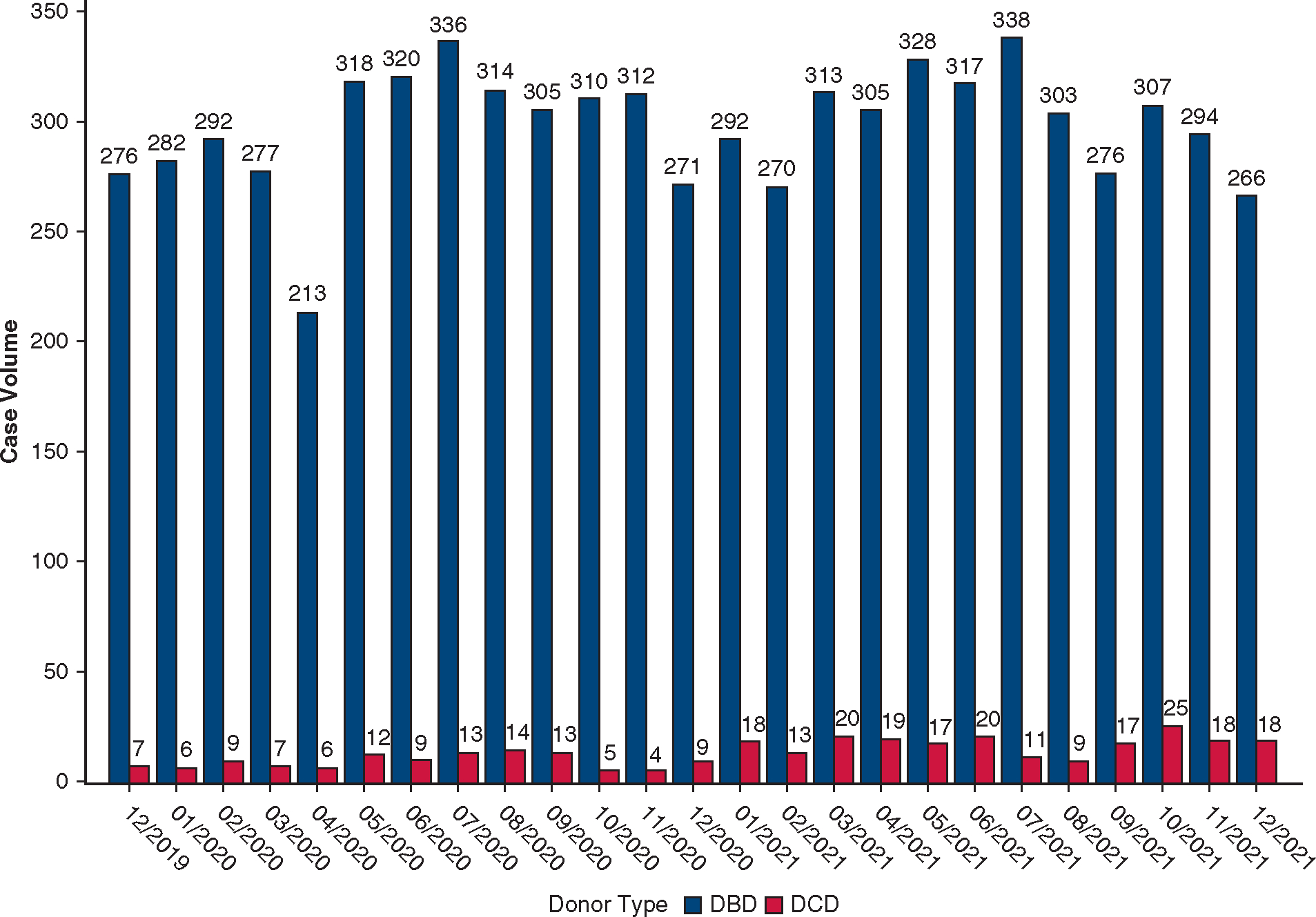
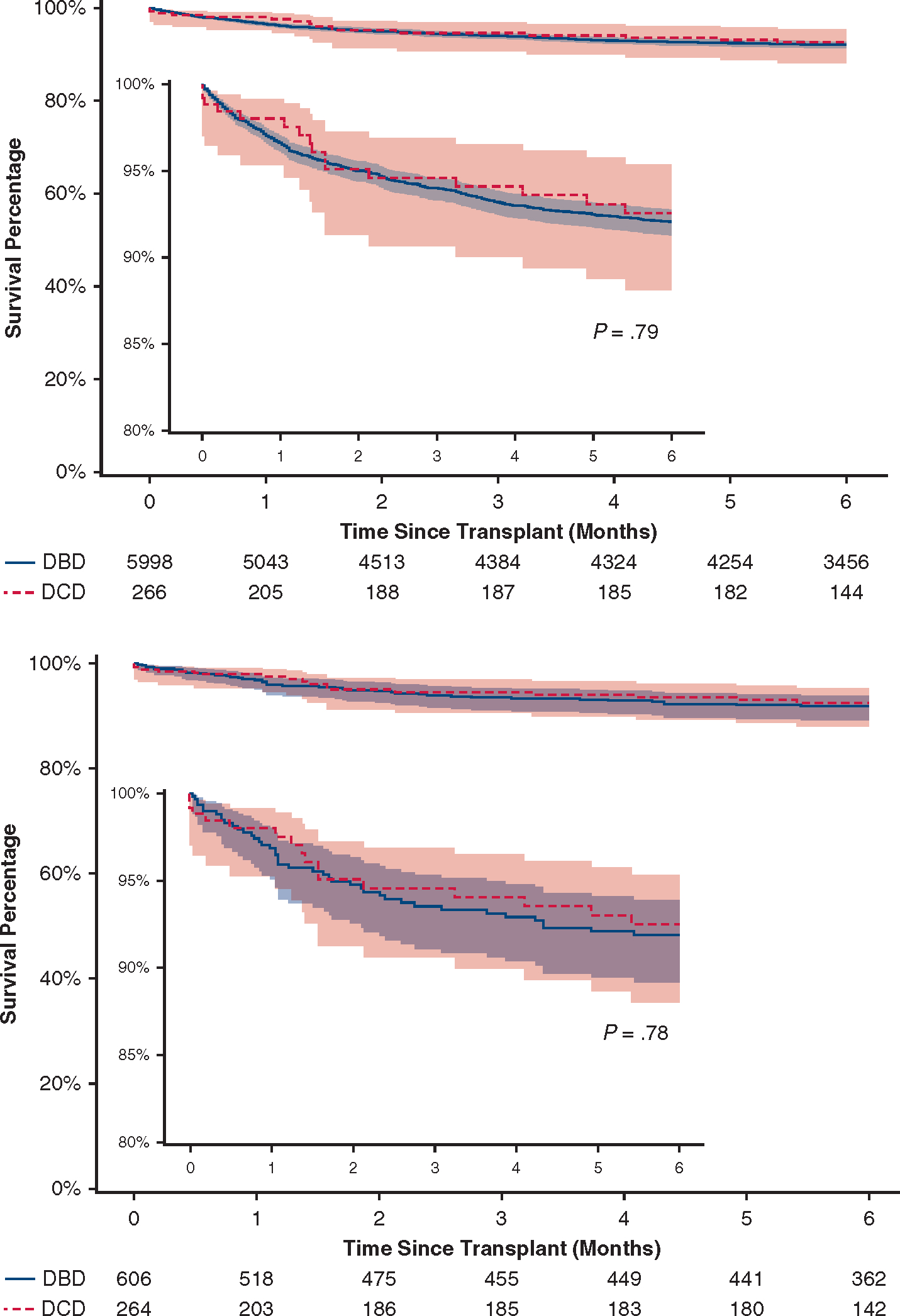
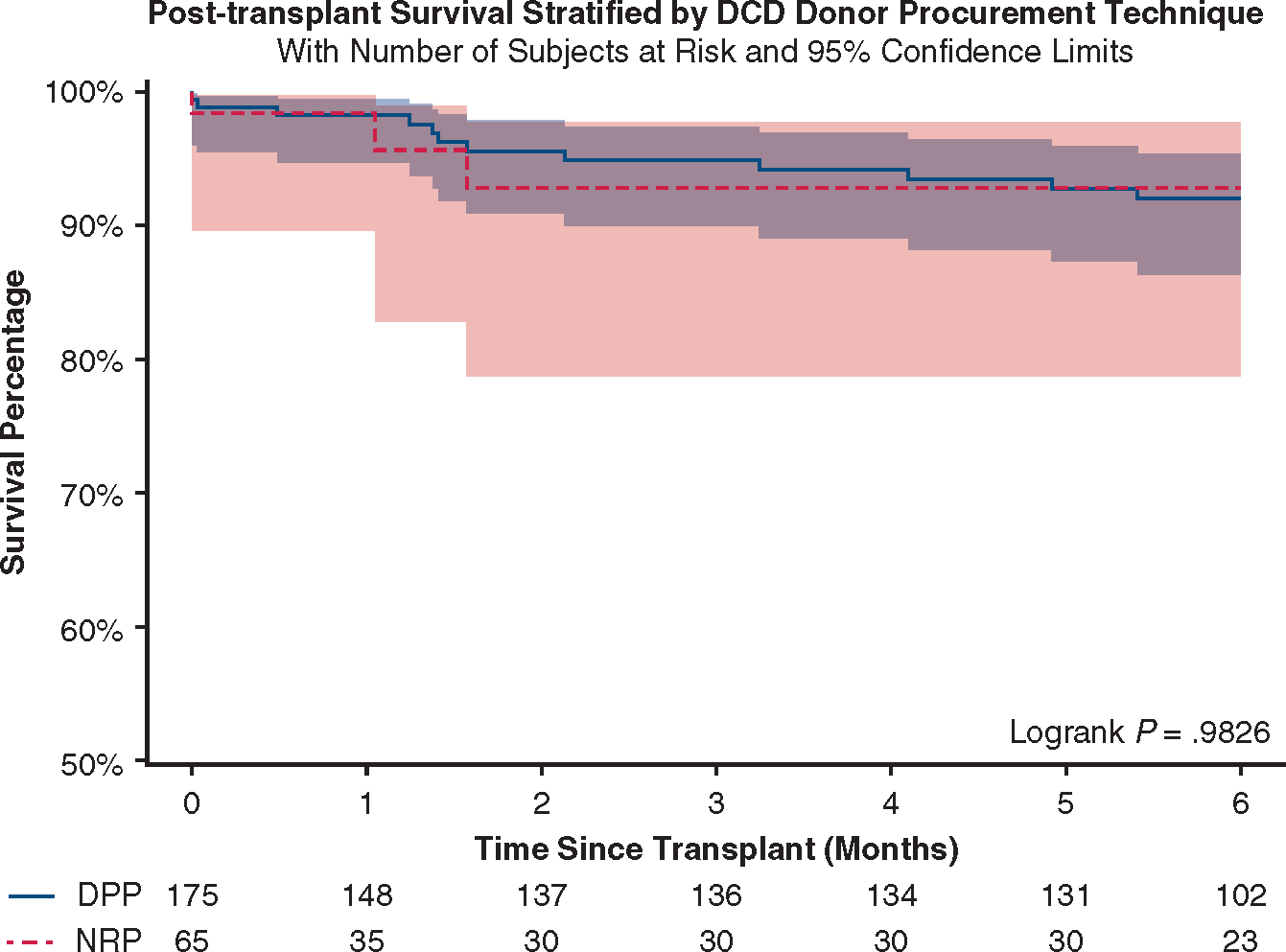
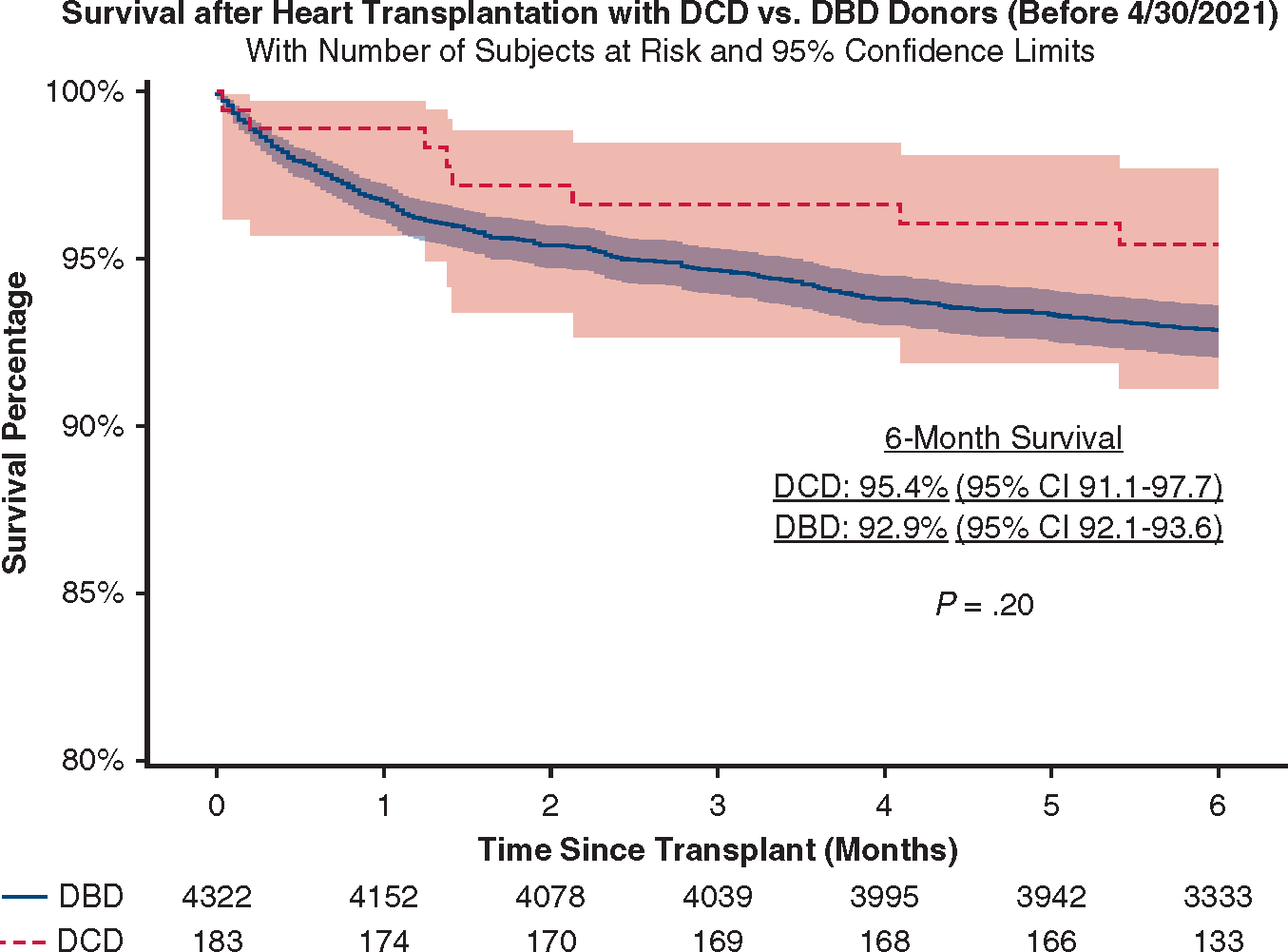
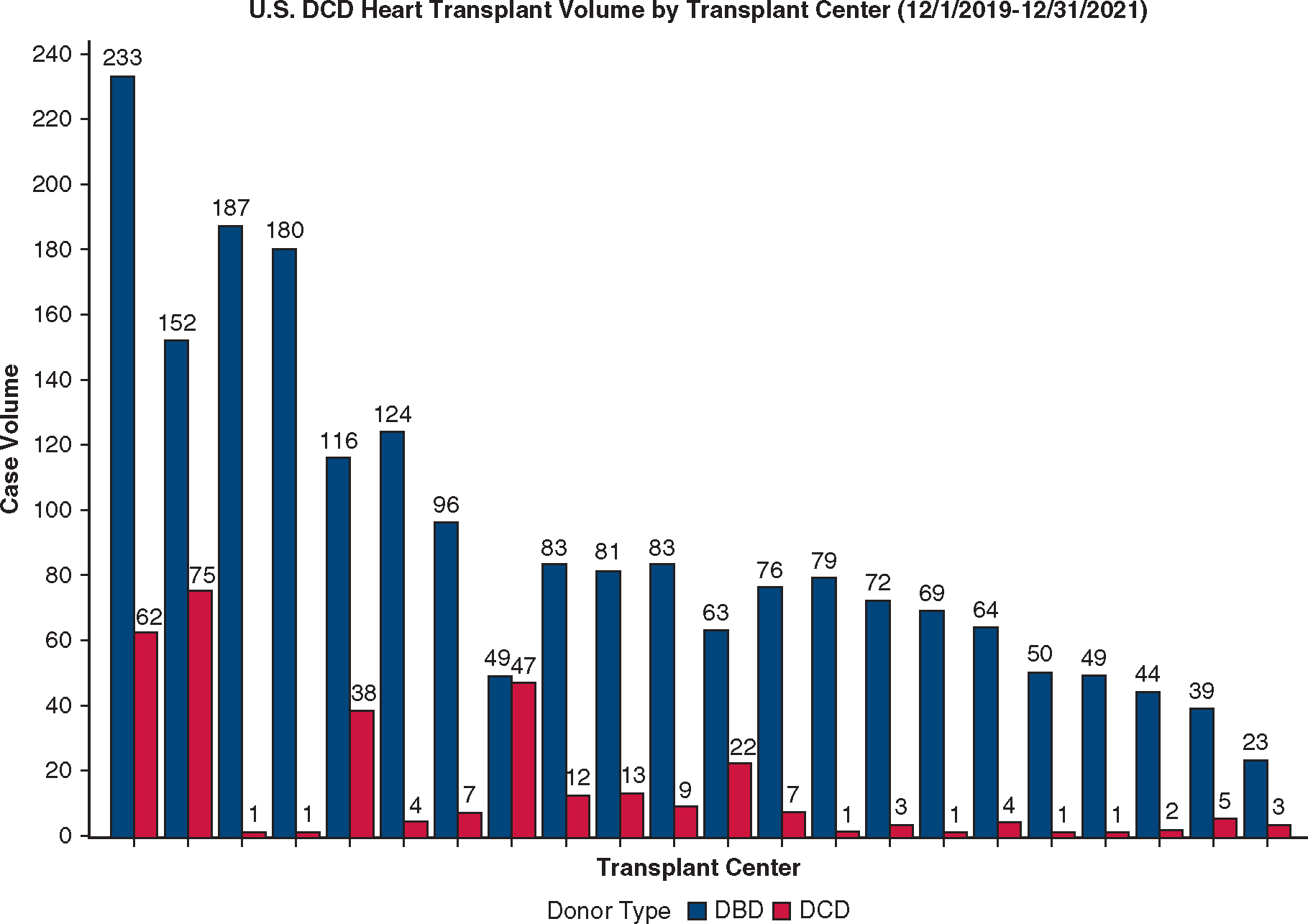
The monthly percentage of donation after circulatory death heart transplant increased from 2.5% in December 2019 to 6.8% in December 2021 (P < .001). Twenty-two centers performed donation after circulatory death heart transplants, ranging from 1 to 75 transplants per center. Four centers performed 70% of the national volume. Recipients of donation after circulatory death hearts were more likely to be clinically stable (80.4% vs 41.1% in status 3-6, P < .001), to have type O blood (58.3% vs 39.9%, P < .001), and to wait longer after listing (55, interquartile range, 15-180 days vs 32, interquartile range, 9-160 days, P = .003). Six-month survival was 92.1% (95% confidence interval, 91.3-92.8) after donation after brain death heart transplants and 92.6% (95% confidence interval, 88.1-95.4) after donation after circulatory death heart transplants (hazard ratio, 0.94, 95% confidence interval, 0.57-1.54, P = .79). Outcomes in propensity-matched patients were similar except for higher rates of treated acute rejection in donation after circulatory death transplants before discharge (14.4% vs 8.8%, P = .01). In donation after circulatory death heart recipients, outcomes did not differ based on the procurement technique (normothermic regional perfusion vs direct procurement and perfusion).
Heart transplantation with donation after circulatory death donors has short-term survival comparable to donation after brain death transplants. Broader implementation could substantially increase donor organ availability.
在美国,心脏停跳后捐献最近被重新引入,希望增加供体心脏的可用性。我们研究了其全国使用情况和结果。
利用美国器官共享网络数据库,确定 2019 年 12 月 1 日至 2021 年 12 月 31 日期间,在排除心肺移植后,使用心脏停跳后捐献供体(n=266)和脑死亡后捐献供体(n=5998)进行心脏移植的已验证成年患者。使用倾向评分匹配来创建更平衡的组进行比较。
心脏停跳后捐献心脏移植的每月百分比从 2019 年 12 月的 2.5%增加到 2021 年 12 月的 6.8%(P<.001)。有 22 个中心进行了心脏停跳后捐献移植,每个中心的移植数量从 1 例到 75 例不等。有 4 个中心完成了全国 70%的工作量。心脏停跳后捐献心脏的受者更可能处于临床稳定状态(80.4%比状态 3-6的 41.1%,P<.001),更可能是 O 型血(58.3%比 39.9%,P<.001),并且在登记后等待时间更长(55,四分位间距,15-180 天与 32,四分位间距,9-160 天,P=.003)。脑死亡后心脏移植的 6 个月生存率为 92.1%(95%置信区间,91.3-92.8),心脏停跳后捐献心脏移植的 6 个月生存率为 92.6%(95%置信区间,88.1-95.4)(风险比,0.94,95%置信区间,0.57-1.54,P=.79)。倾向评分匹配患者的结果相似,但心脏停跳后捐献移植的出院前治疗性急性排斥反应发生率较高(14.4%比 8.8%,P=.01)。在心脏停跳后捐献心脏受者中,基于采集技术(常温区域性灌注与直接采集和灌注),结果无差异。
心脏停跳后捐献供体的心脏移植具有与脑死亡移植相当的短期生存率。更广泛的实施可以大大增加供体器官的可用性。