Zhang Jian, Wei Zheng-Jun, Wang Hang, Yu Yan-Bing, Sun Hong-Tao
Tianjin Key Laboratory of Neurotrauma Repair, Institute of Traumatic Brain Injury and Neuroscience, Characteristic Medical Center of Chinese People's Armed Police Force, Tianjin 300162, China.
Department of Neurosurgery, China-Japan Friendship Hospital, Beijing 100069, China.
World J Clin Cases. 2022 Jul 16;10(20):7138-7146. doi: 10.12998/wjcc.v10.i20.7138.
Aneurysm compression, diabetes, and traumatic brain injury are well-known causative factors of oculomotor nerve palsy (ONP), while cases of ONP induced by neurovascular conflicts have rarely been reported in the medical community. Here, we report a typical case of ONP caused by right posterior cerebral artery (PCA) compression to increase neurosurgeons' awareness of the disease and reduce misdiagnosis and recurrence.
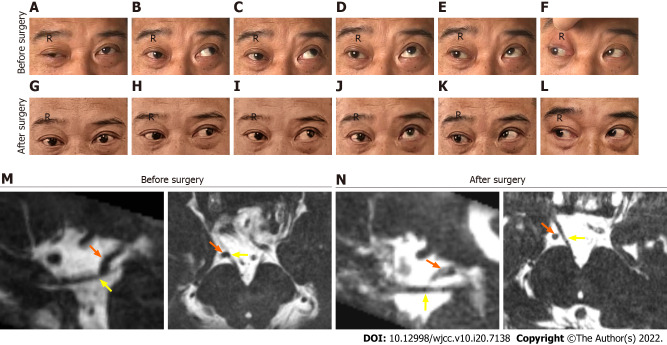
A 54-year-old man without a known medical history presented with right ONP for the past 5 years. The patient presented to the hospital with right ptosis, diplopia, anisocoria (rt 5 mm, lt 2.5 mm), loss of duction in all directions, abduction, and light impaired pupillary reflexes. Magnetic resonance angiography and computed tomography venography examinations showed no phlebangioma, aneurysm, or intracranial lesion. After conducting oral glucose tolerance and prostigmin tests, diabetes and myasthenia gravis were excluded. Cranial nerve magnetic resonance imaging showed that the right PCA loop was in direct contact with the cisternal segment of the right oculomotor nerve (ON). Microvascular decompression (MVD) of the culprit vessel from the ON through a right subtemporal craniotomy was carried out, and the ONP symptoms were significantly relieved after 3 mo.
Vascular compression of the ON is a rare pathogeny of ONP that may be refractory to drug therapy and ophthalmic strabismus surgery. MVD is an effective treatment for ONP induced by neurovascular compression.
动脉瘤压迫、糖尿病和创伤性脑损伤是动眼神经麻痹(ONP)的常见致病因素,而神经血管冲突引起的ONP病例在医学界鲜有报道。在此,我们报告一例由右侧大脑后动脉(PCA)压迫导致的典型ONP病例,以提高神经外科医生对该病的认识,减少误诊和复发。
一名54岁无已知病史男性,过去5年出现右侧ONP。患者因右侧上睑下垂、复视、瞳孔不等大(右侧5mm,左侧2.5mm)、各方向眼球运动障碍、外展及瞳孔对光反射减弱入院。磁共振血管造影和计算机断层扫描静脉造影检查未发现静脉血管瘤、动脉瘤或颅内病变。进行口服葡萄糖耐量试验和新斯的明试验后,排除糖尿病和重症肌无力。颅神经磁共振成像显示右侧PCA袢与右侧动眼神经(ON)脑池段直接接触。通过右侧颞下入路对责任血管进行微血管减压(MVD),术后3个月ONP症状明显缓解。
动眼神经血管压迫是ONP的一种罕见病因,可能对药物治疗和眼科斜视手术无效。MVD是治疗神经血管压迫所致ONP的有效方法。