Department of Hepatobiliary Surgery, The First Affiliated Hospital of Xi'an Jiaotong University, Xi'an, 710061, Shaanxi, China.
Department of General Surgery, The First Affiliated Hospital of Xi'an Jiaotong University, 277 Yanta West Road, Xi'an, 710061, China.
Aging Clin Exp Res. 2022 Dec;34(12):2993-3004. doi: 10.1007/s40520-022-02236-3. Epub 2022 Sep 2.
Sepsis-induced acute kidney injury (S-AKI) is a significant complication and is associated with an increased risk of mortality, especially in elderly patients with sepsis. However, there are no reliable and robust predictive models to identify high-risk patients likely to develop S-AKI. We aimed to develop a nomogram to predict S-AKI in elderly sepsis patients and help physicians make personalized management within 24 h of admission.
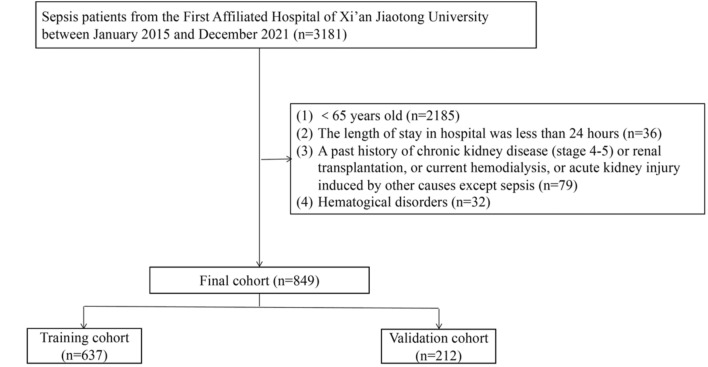
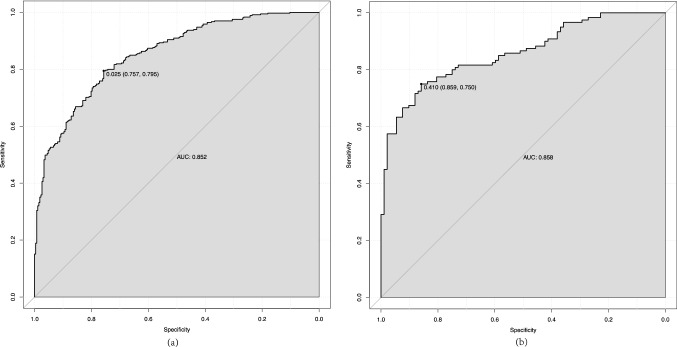
A total of 849 elderly sepsis patients from the First Affiliated Hospital of Xi'an Jiaotong University were identified and randomly divided into a training set (75%, n = 637) and a validation set (25%, n = 212). Univariate and multivariate logistic regression analyses were performed to identify the independent predictors of S-AKI. The corresponding nomogram was constructed based on those predictors. The calibration curve, receiver operating characteristics (ROC)curve, and decision curve analysis were performed to evaluate the nomogram. The secondary outcome was 30-day mortality and major adverse kidney events within 30 days (MAKE30). MAKE30 were a composite of death, new renal replacement therapy (RRT), or persistent renal dysfunction (PRD).
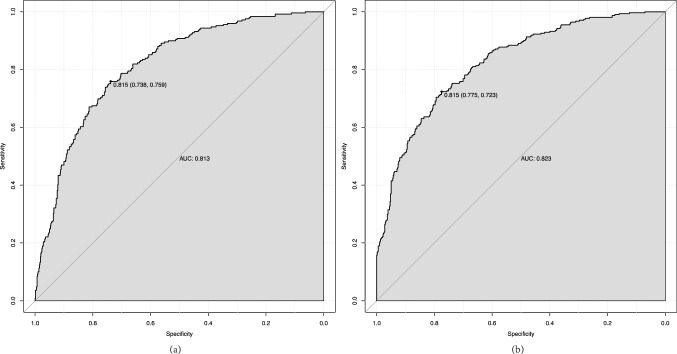
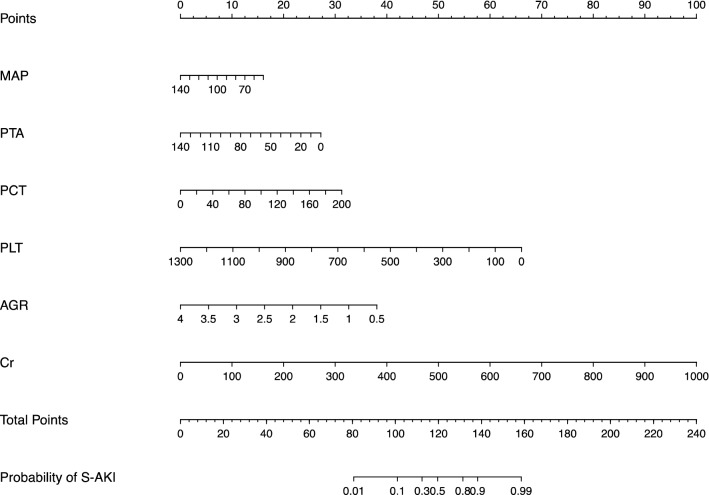
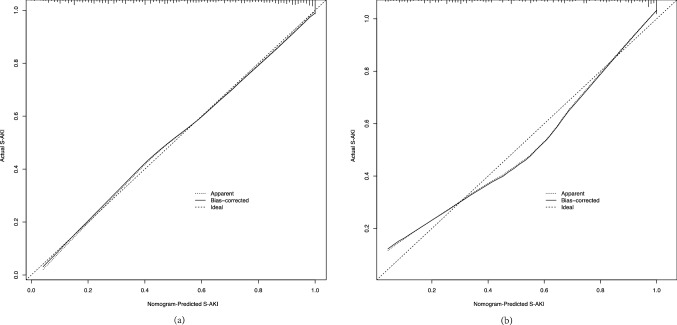
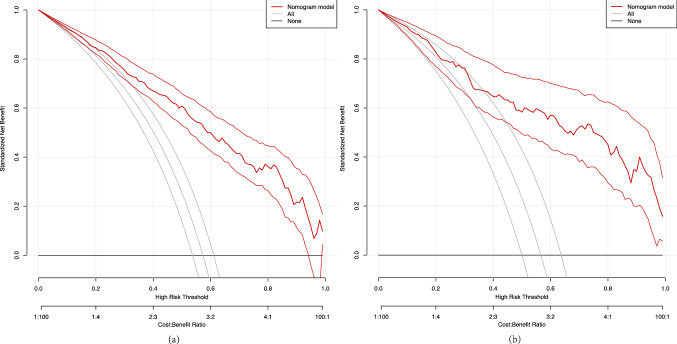
The independent predictors for nomogram construction were mean arterial pressure (MAP), serum procalcitonin (PCT), and platelet (PLT), prothrombin time activity (PTA), albumin globulin ratio (AGR), and creatinine (Cr). The predictive model had satisfactory discrimination with an area under the curve (AUC) of 0.852-0.858 in the training and validation cohorts, respectively. The nomogram showed good calibration and clinical application according to the calibration curve and decision curve analysis. Furthermore, the prediction model had perfect predictive power for predicting 30-day mortality (AUC = 0.813) and MAKE30 (AUC = 0.823) in elderly sepsis patients.
The proposed nomogram can quickly and effectively predict S-AKI risk in elderly sepsis patients within 24 h after admission, providing information for clinicians to make personalized interventions.
脓毒症相关性急性肾损伤(S-AKI)是一种严重的并发症,与死亡率增加相关,尤其是在脓毒症老年患者中。然而,目前尚无可靠且稳健的预测模型来识别可能发生 S-AKI 的高危患者。我们旨在为老年脓毒症患者开发一种列线图来预测 S-AKI,并帮助医生在入院后 24 小时内进行个性化管理。
共纳入 849 例来自西安交通大学第一附属医院的老年脓毒症患者,随机分为训练集(75%,n=637)和验证集(25%,n=212)。进行单因素和多因素逻辑回归分析以确定 S-AKI 的独立预测因素。根据这些预测因素构建相应的列线图。通过校准曲线、接收者操作特征(ROC)曲线和决策曲线分析来评估该列线图。次要结局是 30 天死亡率和 30 天内的主要不良肾脏事件(MAKE30)。MAKE30 是死亡、新的肾脏替代治疗(RRT)或持续肾功能障碍(PRD)的复合结局。
列线图构建的独立预测因素是平均动脉压(MAP)、血清降钙素原(PCT)和血小板(PLT)、凝血酶原时间活动度(PTA)、白蛋白球蛋白比值(AGR)和肌酐(Cr)。预测模型在训练和验证队列中的曲线下面积(AUC)分别为 0.852-0.858,具有良好的区分度。根据校准曲线和决策曲线分析,该列线图显示出良好的校准和临床应用。此外,该预测模型对老年脓毒症患者 30 天死亡率(AUC=0.813)和 MAKE30(AUC=0.823)具有完美的预测能力。
该列线图可以快速有效地预测老年脓毒症患者入院后 24 小时内的 S-AKI 风险,为临床医生提供个性化干预的信息。