Division of Hematology and Oncology, Department of Medicine, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA.
Hospital of the University of Pennsylvania, Philadelphia, PA.
Blood Adv. 2023 May 23;7(10):2132-2142. doi: 10.1182/bloodadvances.2022008443.
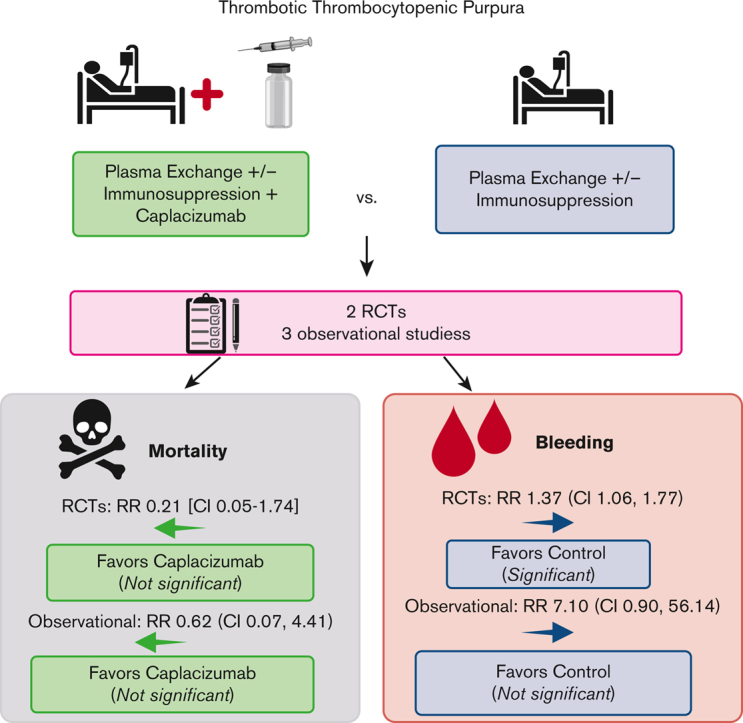
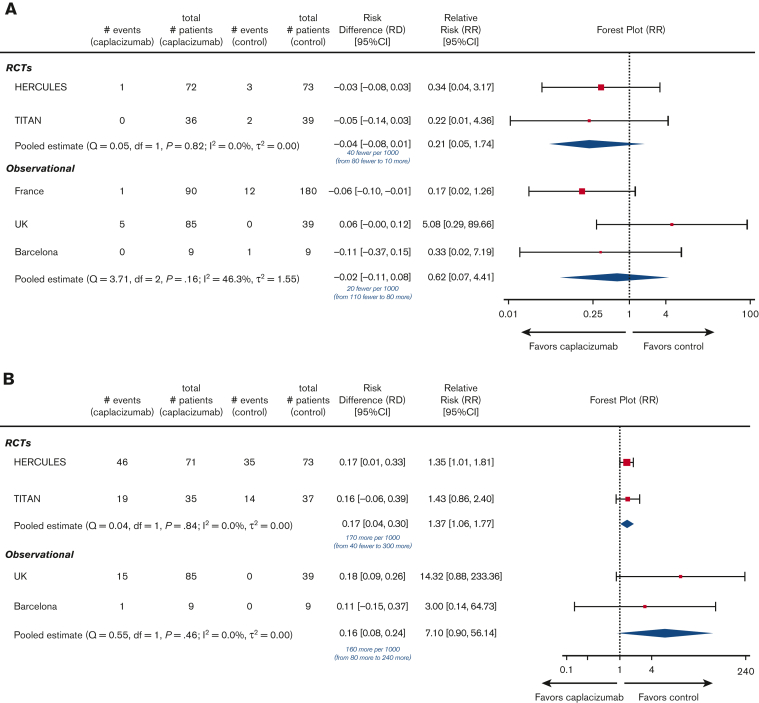
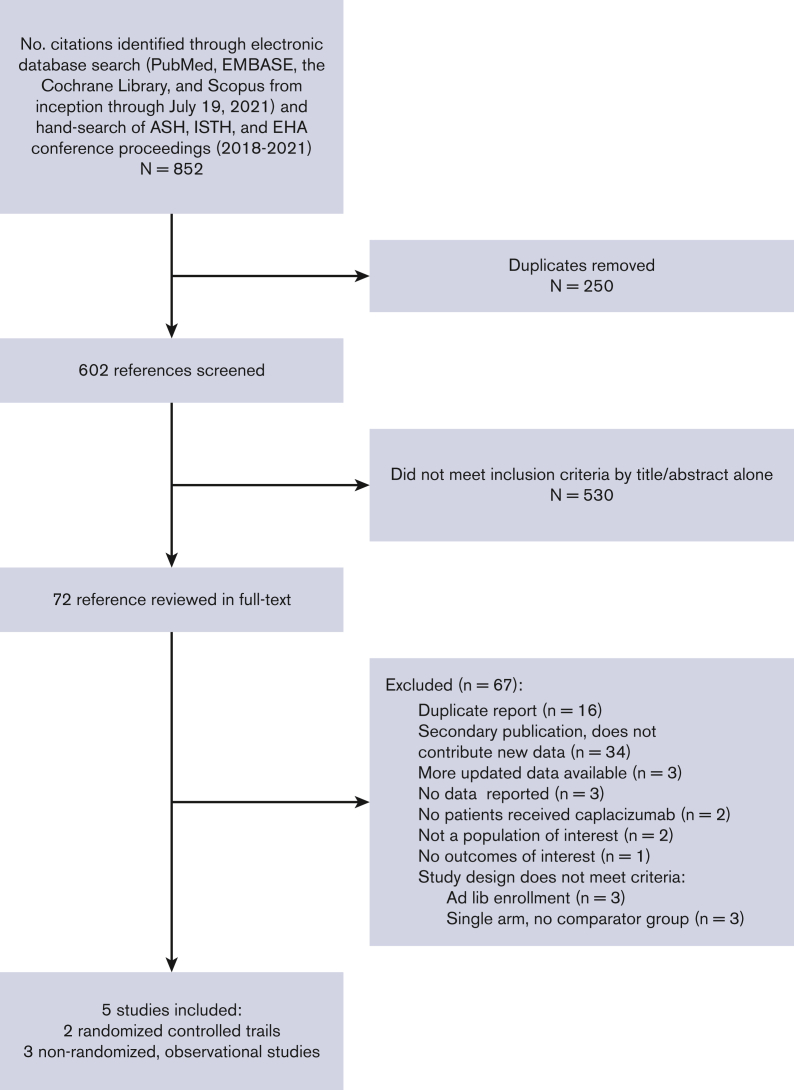
Immune thrombotic thrombocytopenic purpura (iTTP) is an acquired, fatal microangiopathy if untreated. Randomized controlled trials (RCTs) demonstrated faster time to response with addition of caplacizumab to standard of care (SOC). However, concerns about RCT selection bias and the high cost of caplacizumab warrant examination of all evidence, including real-world observational studies. In this systematic review and meta-analysis, we searched for comparative studies evaluating SOC with or without caplacizumab for the treatment of iTTP. We assessed risk of bias using the Cochrane risk-of-bias-2 tool (RCTs) and the Newcastle-Ottawa Scale (observational studies). The primary efficacy and safety outcomes were all-cause mortality and treatment-emergent bleeding, respectively. Secondary outcomes included exacerbation and relapse, refractory iTTP, and time to response. We included 2 high-quality RCTs and 3 observational studies at high risk of bias comprising 632 total participants. Compared with SOC, caplacizumab was associated with a nonsignificant reduction in the relative risk [RR] of death in RCTs (RR, 0.21; 95% confidence interval [CI], 0.05-1.74) and observational studies (RR, 0.62; 95% CI, 0.07-4.41). Compared with SOC, caplacizumab was associated with an increased bleeding risk in RCTs (RR, 1.37; 95% CI, 1.06-1.77). In observational studies, bleeding risk was not significantly increased (RR, 7.10; 95% CI, 0.90-56.14). Addition of caplacizumab was associated with a significant reduction in refractory iTTP and exacerbation risks and shortened response time but increased relapse risk. Frontline addition of caplacizumab does not significantly reduce all-cause mortality compared with SOC alone, although it reduces refractory disease risk, shortens time to response, and improves exacerbation rates at the expense of increased relapse and bleeding risk.
免疫性血栓性血小板减少性紫癜(iTTP)是一种获得性、致命性的微血管病,如果不治疗,病情会迅速恶化。随机对照试验(RCT)表明,与标准治疗(SOC)相比,添加卡普赛珠单抗可更快地获得治疗效果。然而,人们对 RCT 选择偏倚和卡普赛珠单抗高昂成本的担忧,使得我们有必要对所有证据进行评估,包括真实世界的观察性研究。在本系统评价和荟萃分析中,我们检索了评估 SOC 联合或不联合卡普赛珠单抗治疗 iTTP 的比较研究。我们使用 Cochrane 偏倚风险评估工具 2(RCTs)和纽卡斯尔-渥太华量表(观察性研究)来评估偏倚风险。主要疗效和安全性结局分别为全因死亡率和治疗后出血。次要结局包括病情恶化和复发、难治性 iTTP 和反应时间。我们纳入了 2 项高质量的 RCT 和 3 项高偏倚风险的观察性研究,共纳入了 632 名参与者。与 SOC 相比,卡普赛珠单抗在 RCT 中降低了死亡的相对风险(RR,0.21;95%置信区间[CI],0.05-1.74)和观察性研究(RR,0.62;95%CI,0.07-4.41),但无统计学意义。与 SOC 相比,卡普赛珠单抗在 RCT 中增加了出血风险(RR,1.37;95%CI,1.06-1.77),但在观察性研究中,出血风险无显著增加(RR,7.10;95%CI,0.90-56.14)。添加卡普赛珠单抗可显著降低难治性 iTTP 和病情恶化的风险,并缩短反应时间,但增加了复发风险。与 SOC 相比,卡普赛珠单抗作为一线治疗药物不能显著降低全因死亡率,但可以降低难治性疾病的风险,缩短反应时间,提高病情恶化的发生率,但其代价是增加了复发和出血的风险。