Donner Daniel G, Bloom Jason E, Shihata Waled A, Brown Aascha A, Cook Rosalind, Yee Tai Tsin, Lambert Gavin W, Chu Po-Yin, Chan William, Stub Dion, Wang Bing H, Kaye David M
Baker Heart and Diabetes Institute, Melbourne, Australia.
Department of Cardiometabolic Health, University of Melbourne, Melbourne, Australia.
Resusc Plus. 2022 Aug 26;11:100292. doi: 10.1016/j.resplu.2022.100292. eCollection 2022 Sep.
Adrenaline is routinely administered during cardiac arrest resuscitation. Using a novel murine model of cardiac arrest, this study evaluates the effects of adrenaline use on survival and end-organ injury.
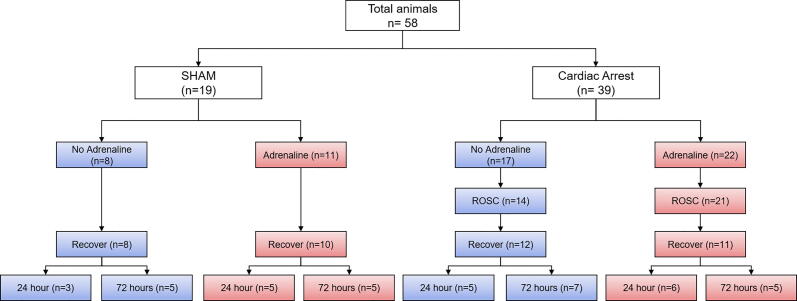
A total of 58 mice, including cardiac arrest (CA) and sham (SHAM) groups received intravenous potassium chloride either as a bolus (CA) or slow infusion (SHAM), inducing ECG-confirmed asystole (in CA only) for 4-minutes prior to intravenous adrenaline (+ADR;250 ul,32 ug/ml) or saline (-ADR;250 ul) and manual chest compressions (300 BPM) for 4-minutes. Mice with return of spontaneous circulation (ROSC) were assessed at 24- or 72-h timepoints.
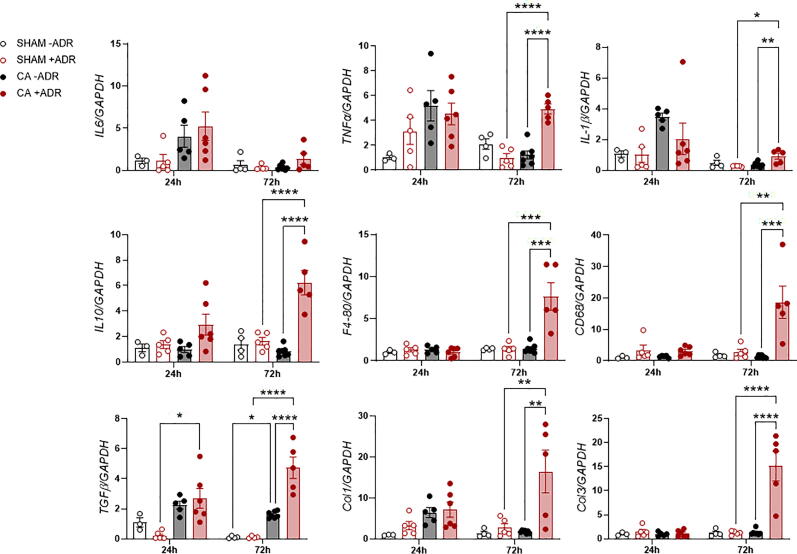
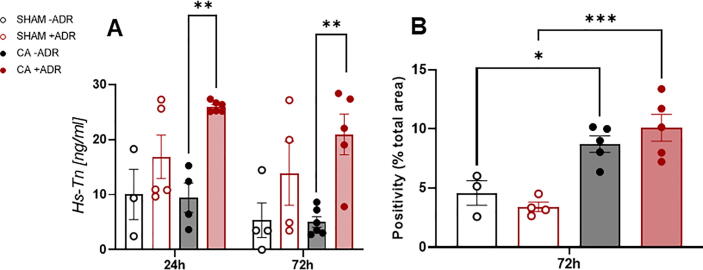
Among animals that underwent CA, rates of ROSC ( = 21 (95 %) vs = 14 (82 %), = 0.18) and survival to the planned endpoint ( = 11 (50 %) vs = 12 (71 %), = 0.19) were similar when comparing those treated with (CA+ADR) and without (CA-ADR) adrenaline. However, in CA animals that initially achieved ROSC, subsequent mortality was approximately 3-fold greater with adrenaline treatment (48 % vs 14 %, = 0.042). Among SHAM animals, adrenaline use had no impact on survival rates or other endpoints. Greater myocardial injury occurred in CA+ADR vs CA-ADR, with increased Hs-Troponin levels measured at 24- (26.0 ± 0.9 vs 9.4 ± 5.3 ng/mL, = 0.015) and 72-h (20.9 ± 8.3 vs 5.0 ± 2.4 ng/mL, = 0.012), associated with increased expression of pro-inflammatory and fibrotic genes within cardiac and renal tissue.
Adrenaline did not improve ROSC or overall survival but following successful ROSC, its use resulted in 3-fold greater mortality rates. Adrenaline was also associated with increased myocardial injury, end-organ inflammation, and fibrosis. These findings underscore the need for further preclinical evaluation of alternate pharmacologic adjuncts for cardiopulmonary resuscitation that improve survival and limit end-organ injury.
在心脏骤停复苏期间常规使用肾上腺素。本研究使用一种新型的心脏骤停小鼠模型,评估使用肾上腺素对生存及终末器官损伤的影响。
总共58只小鼠,包括心脏骤停(CA)组和假手术(SHAM)组,分别接受静脉推注氯化钾(CA组)或缓慢输注氯化钾(SHAM组),诱导心电图确认的心脏停搏(仅CA组)4分钟,然后静脉注射肾上腺素(+ADR;250 μl,32 μg/ml)或生理盐水(-ADR;250 μl),并进行4分钟的手动胸外按压(300次/分钟)。恢复自主循环(ROSC)的小鼠在24小时或72小时时间点进行评估。
在经历心脏骤停的动物中,比较使用肾上腺素治疗的(CA+ADR)和未使用肾上腺素治疗的(CA-ADR)动物,ROSC率(分别为21只(9