National Clinical Research Center for Hematologic Diseases, Jiangsu Institute of Hematology, The First Affiliated Hospital of Soochow University, Suzhou, China.
Institute of Blood and Marrow Transplantation, Collaborative Innovation Center of Hematology, Soochow University, Suzhou, China.
Front Immunol. 2022 Aug 17;13:969660. doi: 10.3389/fimmu.2022.969660. eCollection 2022.
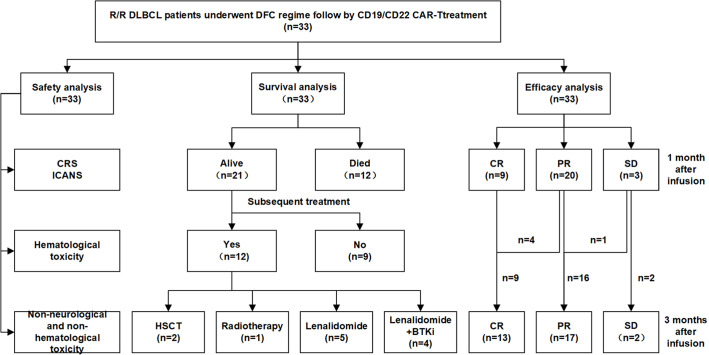
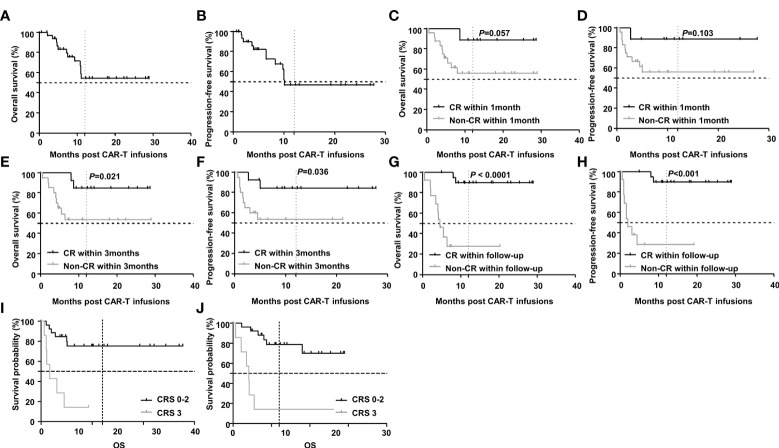
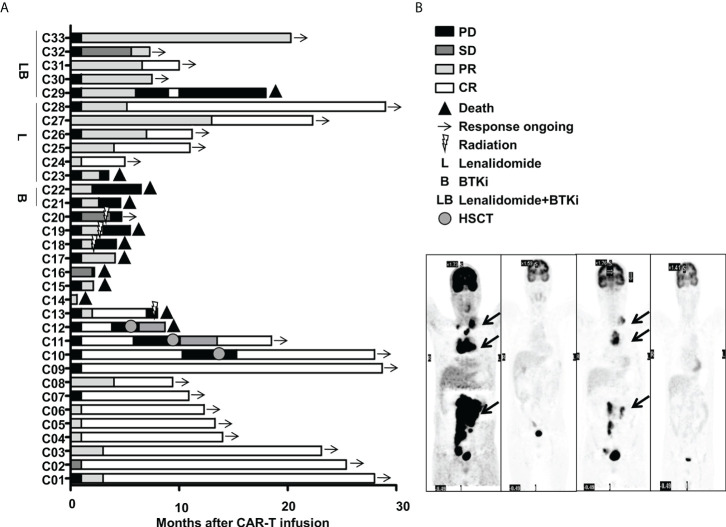
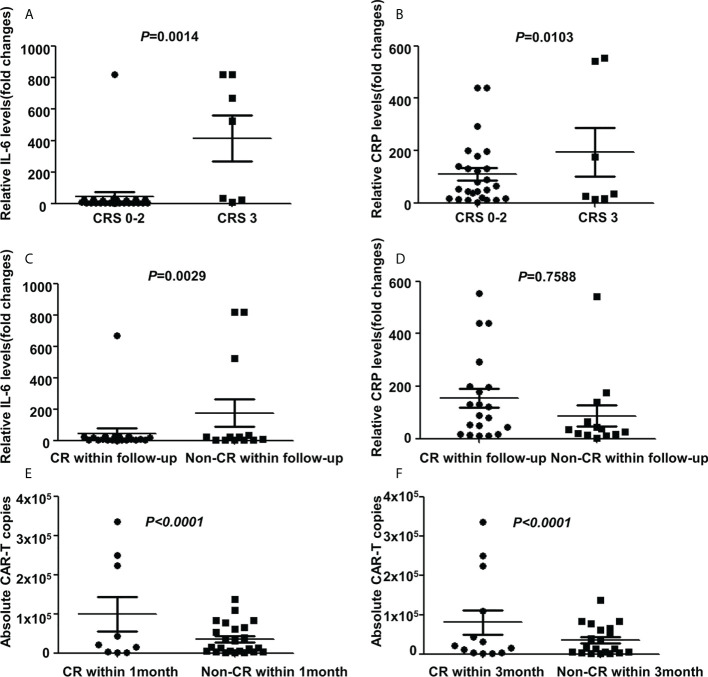
Chimeric antigen receptor T cell (CAR-T) therapy has emerged as highly effective in relapsed/refractory (R/R) diffuse large B-cell lymphoma (DLBCL), but only about 40% patients have achieved sustained responses. Here, we conducted a phase II clinical trial testing efficacy and toxicities of CAR-T therapy in R/R non-Hodgkin's lymphoma patients (NCT03196830). Among enrolled patients, 33 R/R DLBCL patients pretreated with DFC (decitabine, fludarabine plus cyclophosphamide) lymphodepletion chemotherapy and infused with tandem CD19-CD22 based CAR-T cells were drawn out for efficacy and toxicities of CAR-T therapy evaluation. With a median follow-up of 10.9(0.6-29.0) months, the best overall response and complete remission (CR) rates were 90.9% and 63.6%, respectively. The median progression-free survival (PFS) was 10.2 months and overall survival (OS) was undefined. The 2-year OS and PFS rates were 54.3% and 47.2%, respectively. No severe grade 4 cytokine release syndrome (CRS) was observed and grade 3 CRS was observed in only 7 patients; 3 patients developed mild immune effect or cell-associated neurotoxic syndrome. All toxicities were transient and reversible and no CAR-T-related mortality. Further subgroup analysis showed that achieving CR was an independent prognostic factor associated with favorable PFS and OS. The 2-year OS and PFS for patients who achieved CR within 3 months (undefined versus undefined =0.021 and undefined versus undefined =0.036) or during the follow-up period were significantly longer than those who did not (undefined versus 4.6 months < 0.0001 and undefined versus 2.0months <0.001). While severe CRS was also an independent prognostic factor but associated with inferior PFS and OS. The 2-year OS and PFS for patients with grade 3 CRS were significantly shorter than those with grade 0-2 CRS (4.1 months versus undefined <0.0001 and 1.7 months versus undefined =0.0002). This study indicated that CD19/CD22 dual-targeted CAR-T therapy under a decitabine-containing lymphodepletion regimen may be a safe, potent effective approach to R/R DLBCL patients.
嵌合抗原受体 T 细胞(CAR-T)疗法在复发/难治性(R/R)弥漫性大 B 细胞淋巴瘤(DLBCL)中显示出高度有效性,但只有约 40%的患者获得了持续缓解。在这里,我们进行了一项 II 期临床试验,以测试 R/R 非霍奇金淋巴瘤患者的 CAR-T 疗法的疗效和毒性(NCT03196830)。在入组的患者中,33 例 R/R DLBCL 患者在接受 DFC(地西他滨、氟达拉滨加环磷酰胺)淋巴细胞耗竭化疗预处理后输注串联 CD19-CD22 靶向的 CAR-T 细胞,以评估 CAR-T 疗法的疗效和毒性。中位随访 10.9(0.6-29.0)个月后,最佳总缓解率和完全缓解(CR)率分别为 90.9%和 63.6%。中位无进展生存期(PFS)为 10.2 个月,总生存期(OS)未定义。2 年 OS 和 PFS 率分别为 54.3%和 47.2%。未观察到严重的 4 级细胞因子释放综合征(CRS),仅 7 例患者发生 3 级 CRS;3 例患者发生轻度免疫效应或细胞相关神经毒性综合征。所有毒性均为短暂且可逆的,且无 CAR-T 相关死亡。进一步的亚组分析表明,达到 CR 是与良好的 PFS 和 OS 相关的独立预后因素。3 个月内(未定义与未定义=0.021)或随访期间(未定义与未定义=0.036)达到 CR 的患者 2 年 OS 和 PFS 明显长于未达到 CR 的患者(未定义与 4.6 个月 <0.0001,未定义与 2.0 个月 <0.001)。虽然严重的 CRS 也是一个独立的预后因素,但与较差的 PFS 和 OS 相关。3 级 CRS 患者的 2 年 OS 和 PFS 明显短于 0-2 级 CRS 患者(4.1 个月与未定义 <0.0001,1.7 个月与未定义=0.0002)。这项研究表明,基于含地西他滨的淋巴细胞耗竭方案的 CD19/CD22 双靶向 CAR-T 疗法可能是一种安全、有效的治疗 R/R DLBCL 患者的方法。