Clinical Research Division, Fred Hutchinson Cancer Research Center, Seattle, WA.
Division of Medical Oncology, Department of Medicine, University of Washington, Seattle, WA.
Blood. 2020 May 7;135(19):1650-1660. doi: 10.1182/blood.2019002936.
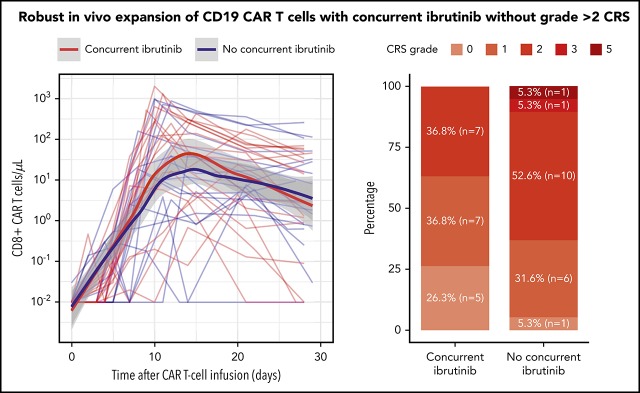
We previously reported durable responses in relapsed or refractory (R/R) chronic lymphocytic leukemia (CLL) patients treated with CD19-targeted chimeric antigen receptor-engineered (CD19 CAR) T-cell immunotherapy after ibrutinib failure. Because preclinical studies showed that ibrutinib could improve CAR T cell-antitumor efficacy and reduce cytokine release syndrome (CRS), we conducted a pilot study to evaluate the safety and feasibility of administering ibrutinib concurrently with CD19 CAR T-cell immunotherapy. Nineteen CLL patients were included. The median number of prior therapies was 5, and 17 patients (89%) had high-risk cytogenetics (17p deletion and/or complex karyotype). Ibrutinib was scheduled to begin ≥2 weeks before leukapheresis and continue for ≥3 months after CAR T-cell infusion. CD19 CAR T-cell therapy with concurrent ibrutinib was well tolerated; 13 patients (68%) received ibrutinib as planned without dose reduction. The 4-week overall response rate using 2018 International Workshop on CLL (iwCLL) criteria was 83%, and 61% achieved a minimal residual disease (MRD)-negative marrow response by IGH sequencing. In this subset, the 1-year overall survival and progression-free survival (PFS) probabilities were 86% and 59%, respectively. Compared with CLL patients treated with CAR T cells without ibrutinib, CAR T cells with concurrent ibrutinib were associated with lower CRS severity and lower serum concentrations of CRS-associated cytokines, despite equivalent in vivo CAR T-cell expansion. The 1-year PFS probabilities in all evaluable patients were 38% and 50% after CD19 CAR T-cell therapy, with and without concurrent ibrutinib, respectively (P = .91). CD19 CAR T cells with concurrent ibrutinib for R/R CLL were well tolerated, with low CRS severity, and led to high rates of MRD-negative response by IGH sequencing.
我们之前报道过,在伊布替尼治疗失败后,接受 CD19 靶向嵌合抗原受体工程(CD19 CAR)T 细胞免疫疗法治疗的复发或难治性(R/R)慢性淋巴细胞白血病(CLL)患者中,有持久缓解的病例。由于临床前研究表明,伊布替尼可以提高 CAR T 细胞的抗肿瘤疗效,并减少细胞因子释放综合征(CRS),因此我们进行了一项初步研究,以评估在给予 CD19 CAR T 细胞免疫疗法的同时给予伊布替尼的安全性和可行性。该研究纳入了 19 例 CLL 患者。患者之前接受的中位数治疗次数为 5 次,且 17 例(89%)患者存在高危细胞遗传学异常(17p 缺失和/或复杂核型)。伊布替尼计划在白细胞分离术之前开始至少 2 周,并在 CAR T 细胞输注后继续使用至少 3 个月。CD19 CAR T 细胞与伊布替尼同时治疗的患者耐受性良好;13 例(68%)患者按计划接受了伊布替尼治疗,未减少剂量。按照 2018 年国际慢性淋巴细胞白血病研讨会(iwCLL)标准,4 周总缓解率为 83%,61%的患者通过 IGH 测序达到了骨髓微小残留病(MRD)阴性反应。在这部分患者中,1 年的总生存率和无进展生存率(PFS)分别为 86%和 59%。与未接受伊布替尼治疗的 CAR T 细胞治疗的 CLL 患者相比,尽管 CAR T 细胞体内扩增情况相当,但与伊布替尼同时使用的 CAR T 细胞与较低的 CRS 严重程度和较低的 CRS 相关细胞因子血清浓度相关。所有可评估患者的 1 年 PFS 概率分别为接受 CD19 CAR T 细胞治疗后有和无伊布替尼时的 38%和 50%(P =.91)。对于 R/R CLL,CD19 CAR T 细胞与伊布替尼同时使用的耐受性良好,CRS 严重程度较低,并且通过 IGH 测序达到了很高的 MRD 阴性反应率。